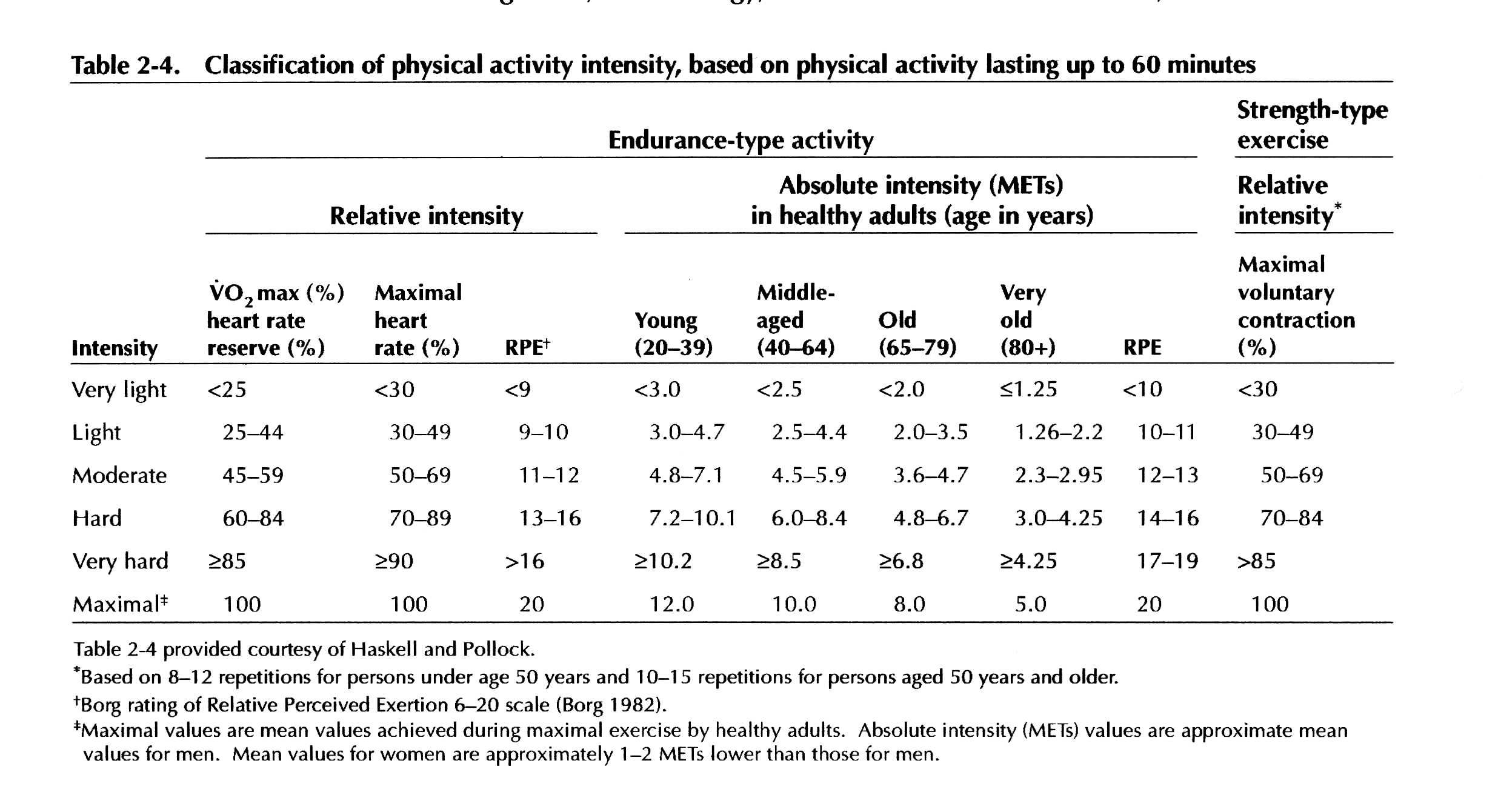
Exercise prescriptions specify values for three parameters: intensity, duration, and frequency. The parameters contribute to a total exercise stimulus called training volume
Course objectives, Control of Human Movement 2
Reading for Control of Human Movement 2:
Full text versions of this article are available through the University's Medline account on OVID (unique identifier 98287757) or by accessing the list of position stands listed at the ACSM web site.
Exercise prescriptions specify values for three parameters: intensity, duration, and frequency. The parameters contribute to a total exercise stimulus called training volume
|
|---|
Therapists can calibrate exercise intensity by establishing a training heart rate at:
examples include: walking-hiking, running-jogging, cycling-bicycling, cross-country skiing, aerobic dance/group exercise, rope skipping, rowing, stair climbing, swimming, skating.
"The most effective exercise prescription begins with a type of aerobic activity the patient enjoys. A prescribed schedule of stepwise increments in frequency, duration, and intensity gradually leads to a maintenance level of fitness (Kligman & Pepin, 1992, p. 33)."
People with type 2 (adult onset) diabetes mellitus (Albright et al., 2000)
Rehabilitation, including aerobic and resistance exercise, for people with neuromuscular diseases, from the Muscular Dystrophy Association (MDA) web site.
Resting heart rate (RHR) training heart rate (THR)
maximum heart rate HRmax reserve (HRR) = MHR-RHR | |||||
|---|---|---|---|---|---|
(0.70) x (220-60) = 112
80 + (0.70) x [(220-60)-80] = 136
While the first equation is easy to teach to patients, applying it to older people can be problematic. In older people, the equation may calculate a THR that is close to the RHR, and imply that the person may exercise at only the most trivial intensities. In these cases, therapists should use the second formula, or have the person judge intensity through a "rating of perceived exertion" (PRE).
How does your exercising | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Very, very light 6 - 8
Very light 9 - 10
Fairly light 11 - 12
Somewhat hard 13 - 14
Hard 15 - 16
Very 17 - 18
Very, very hard 19 - 20 |
|
|---|
American College of Sports Medicine. (1993). American College of Sports Medicine position stand. Physical activity, physical fitness, and hypertension. Medical Science in Sports and Exercise, 25,10, i-x.
American College of Sports Medicine. (1998a). American College of Sports Medicine position stand. Exercise and physical activity for older adults. Medical Science in Sports and Exercise, 30, 992-1008.
American College of Sports Medicine. (1998b). American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Medicine and Science in Sports and Exercise, 30, 975-91.
Dishman, R.K. (1994). Prescribing exercise intensity for healthy adults using perceived exertion. Medicine & Science in Sports & Exercise, 26, 1087-94.
Gutin, B. and Kasper, M.J. (1992). Can vigorous exercise play a role in osteoporosis prevention? A review. Osteoporosis International, 2, 55-69.
Hillegass, E.A., & Sadowsky, H.S. (1994). Essentials of cardiopulmonary physical therapy. Philadelphia: W.B. Saunders.
Karvonen, M., Kentala, K., & Mustala, O. (1957). The effects of training heart rate: A longitudinal study. Annals of Medicine and Experimental Biology Fenn 35, 307-315.
Kligman, E.W., & Pepin, E. (1992). Prescribing physical activity for older patients. Geriatrics, 47(8), 33-4, 37-44, 47.
McArdle, W.D., Katch, F.I., & Katch, V.L. (1996). Exercise physiology: Energy, nutrition, and human performance. Baltimore: Williams and Wilkins.
Nelson, M. E., Dilmanian, F.A., Dallal, G.E., & Evans, W.J. (1991). A one-year walking program and increased dietary calcium in postmenopausal women: Effects on bone. American Journal of Clinical Nutrition, 53, 1304-1311.
U.S. Department of Health and Human Services. (1996). Physical activity and health: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Preventtion, National Center for Chronic Disease Prevention and Health Promotion.