Case No.: D-002
Diagnosis: Ameloblastoma
Organ: Mandible
Last Updated: 09/21/2010
|
|
|
Panoramic view |
 CT |
Gross photo |
|
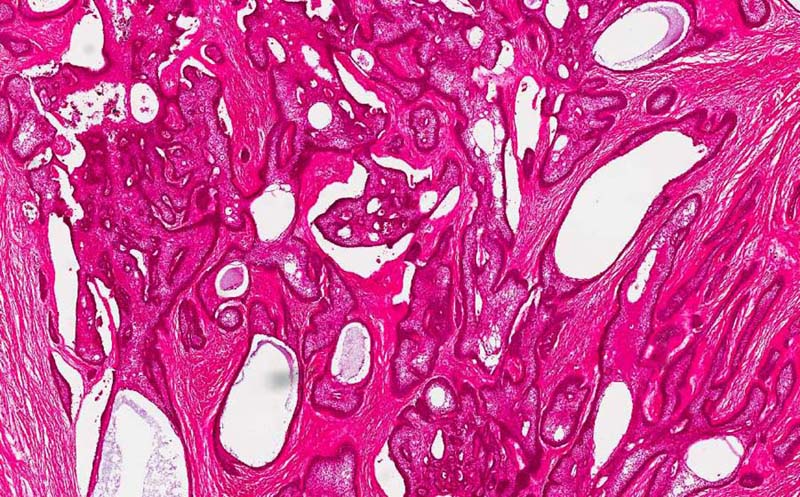
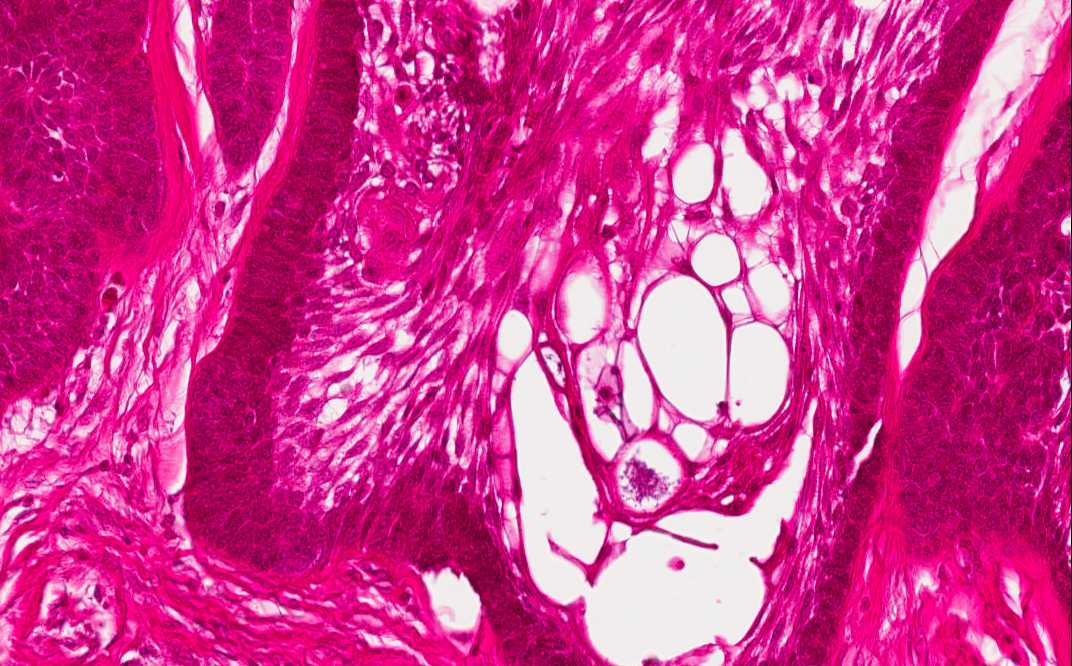
Hematoxylin & eosin |
Area 1: Note that the cords and nests contains peripherally located palisading epithelial cells with reversed polarity. These cells resembles the ameloblasts of normal tooth formation. The stellate central cells resemble the stellate reticulum of the tooth germ. |
|
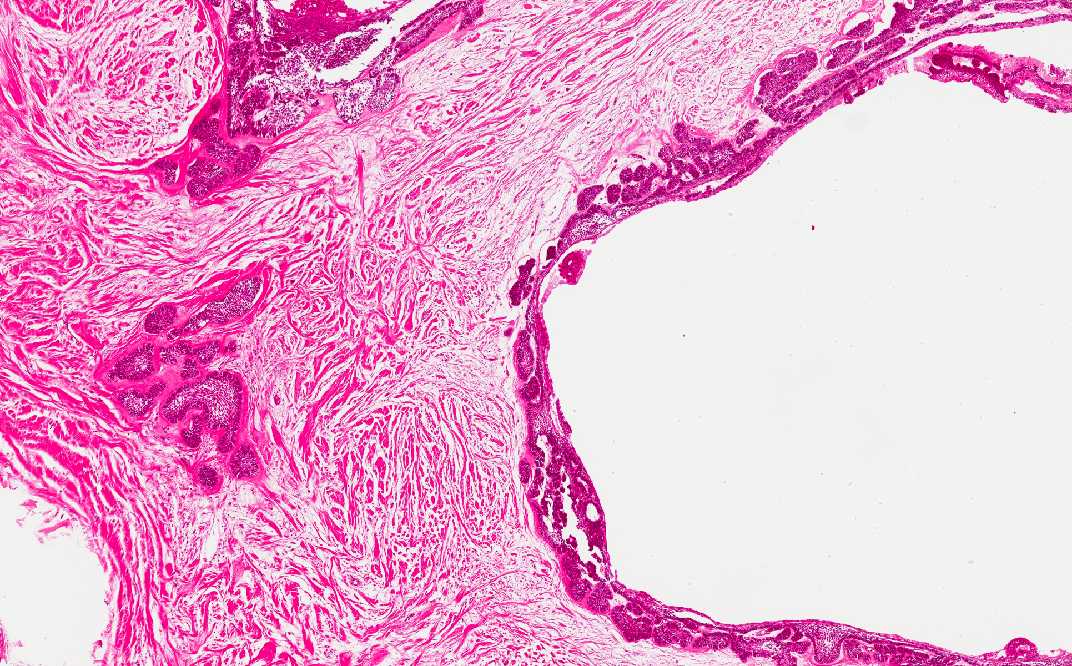
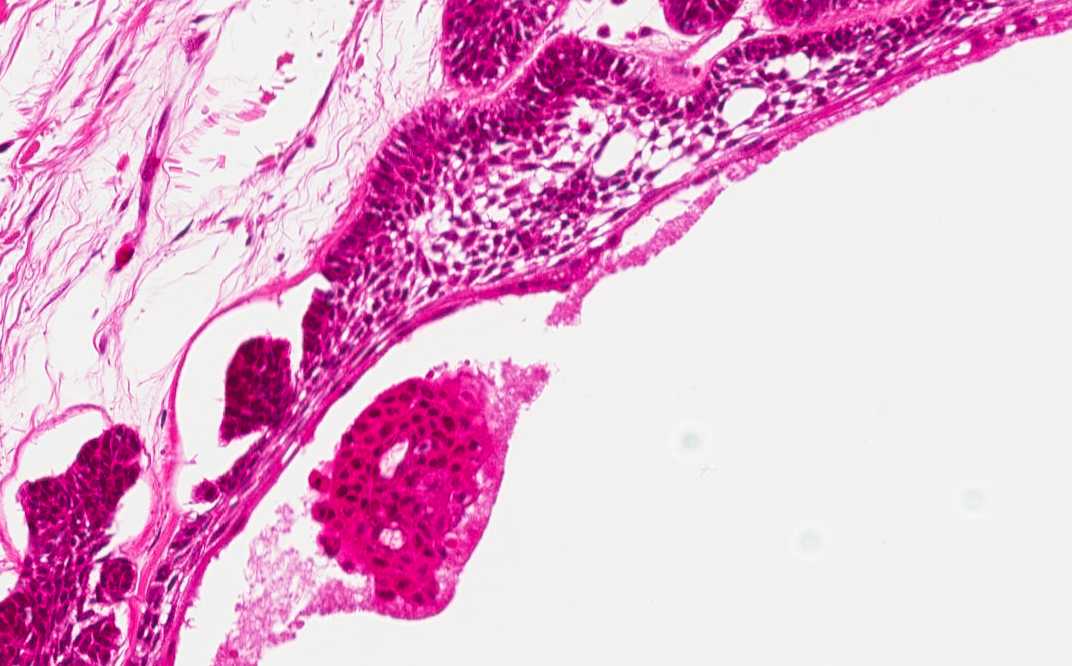
Hematoxylin & eosin |
Area 2: Note that the cyst are lined by palisading columnar cells with reversed polarity. Cyst formation is very common in ameloblastomas. Some of the cyst may be, at least partially, lined by attenuated squamous epithelium that lacks features of ameloblasts. |
|
History: The patient was a 34 year-old man who presented with a 4 day history of pain and swelling, dysphagia, dysphonia, and odynophagia. On physical examination, there was significant swelling with induration on his left face posterior to the ramus of the mandible. The swelling was severely tender on palpation. The swelling extended anterior and inferior to the submandibular space. The inferior border of the mandible could not be palpated. A panoramic film showed a multilocated radiolucent lesion in the left mandible close. An unerupted tooth was present within this lesion. A CT scan showed a large lytic lesion involving the left mandibular body and ramus and rightward shift of airway of inferior oropharynx. The lesion was excised and yielded this specimen.
Imaging Studies: The panoramic view demonstrated a cystic lesion (outlined by the arrow) that greatly expanded the mandibuylar condyle, angle, and ramus. It is an multilocular cys in with thin walled cysts. This "soap bubble" like radiolucency is classic for ameloblastoma. At the base of the lesion is a tooth. It is not uncommon for them to be associated with unerupted tooth. The bone window of the CT scan demonstrated similar findings. Note that the lesion is large enough to compress and deviate the airway (the airway has shifted right). Note that the molar region of mandible is the most common location for ameloblastoma.
Gross Pathology: The resection included the left body, angle, ramus, and condyle of the mandible. The specimen was 4.5 x 4.0 x 2.9 cm. The specimen was decacified for examination. Cross section demonstrated a multilocular cyst with large and small cyst. The tumor is gray white on cut surface.
Histologic Highlights of this Case:
Comment:
|
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.