|
History: This slide was
taken from an old teaching file. The deceased subject was a premature
baby with respiratory distress shortly after birth.
Clinical Perspectives:
-
Hyaline membrane disease is really a morphologic term of diffuse
alveolar injury and it highlights the most prominent feature of this
entity which is the formation of a thin layer of membranous
substance lining the injured alveoli. In clinical manifestation, the
baby will suffer infant respiratory distress syndrome (IRDS) which
is also called surfactant deficiency disorder.
-
It is usually resulted from insufficient surfactant and immaturity
of the lung in premature neonates. It is more common in preterm,
even term neonates of diabetic mothers and in the second born of
premature twins. Premature neonates born at 26-28 weeks of gestation
have about 50% chances to develop IRDS but premature neonates born
at 30-31 weeks of gestation are half as likely to develop this
problem.
-
Classic radiologic findings include ground glass opacity due to
incomplete expansion and less air in the lung. As a result, air
containing bronchus (appears dark because they contains air) will
show up in this relatively solid background (which appears hazy,
ground glass white on plain film) to give a picture of "air
bronchogram". Because of the lack of air, the lung often
appears solid or liver like on gross examination.
-
Mutations of adenosine triphosphate (ATP)–binding cassette gene (ABCA3)
on chromosome 16 result in fatal surfactant deficiency.
-
Mutations of surfactant protein-B gene (SFTPB) on
chromosome 2 leads to a partial or complete absence of surfactant
protein B and is transmitted as an autosomal recessive trait will
cause IRDS.
-
Mutation of
surfactant protein C gene (SFTPC) on chromosome 8 may cause
IRDS and also contribute to chronic lung diseases such as
interstitial lung diseases and emphysema as patients ages.
-
Mutation of
8 could also cause lung diseases but their presentations are more
variable and do not always cause IRDS. Mutation of these genes,
however, may contribute to interstitial lung diseases and emphysema
as patients ages.
Histologic Highlights of this Case:
-
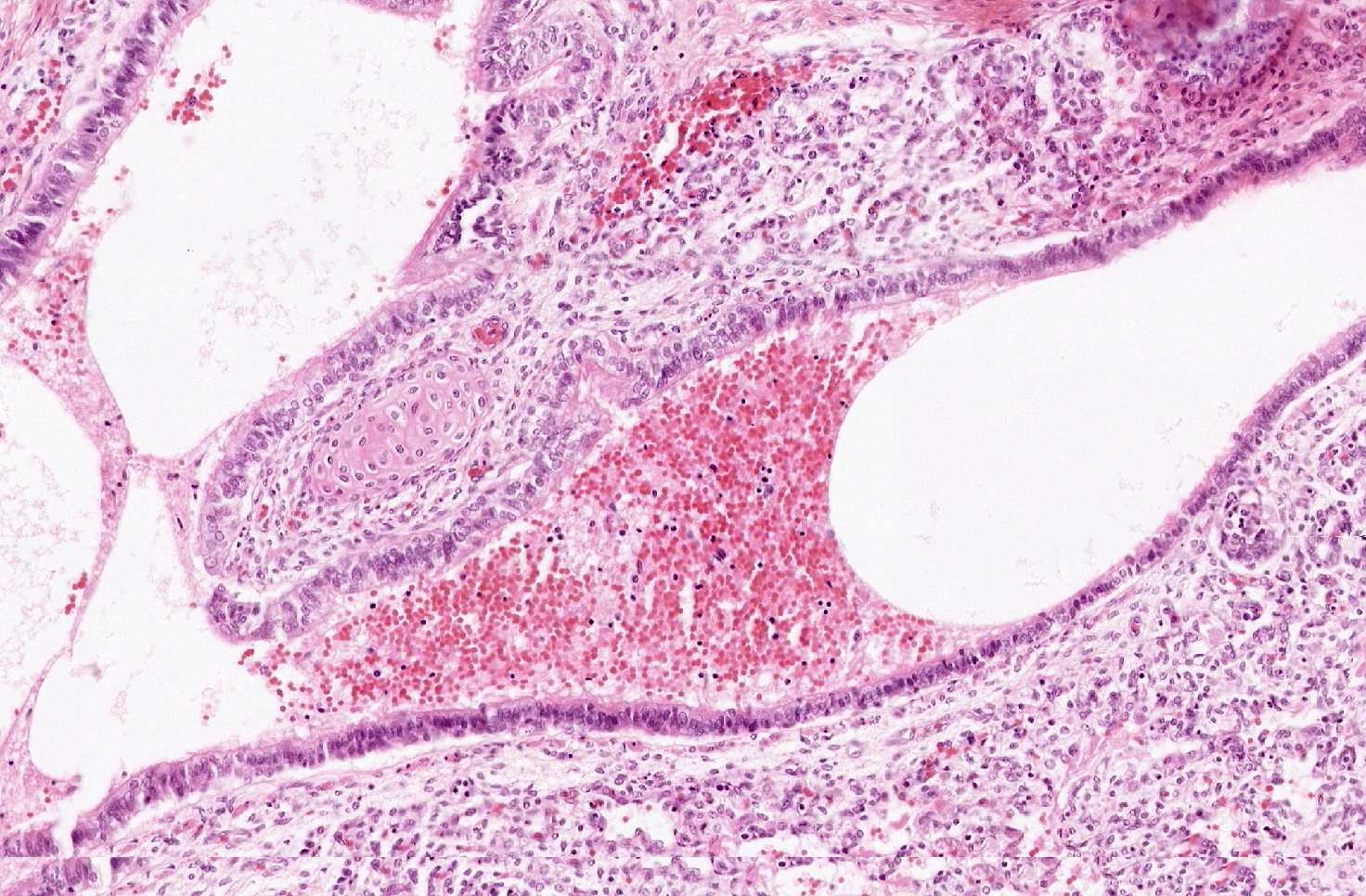
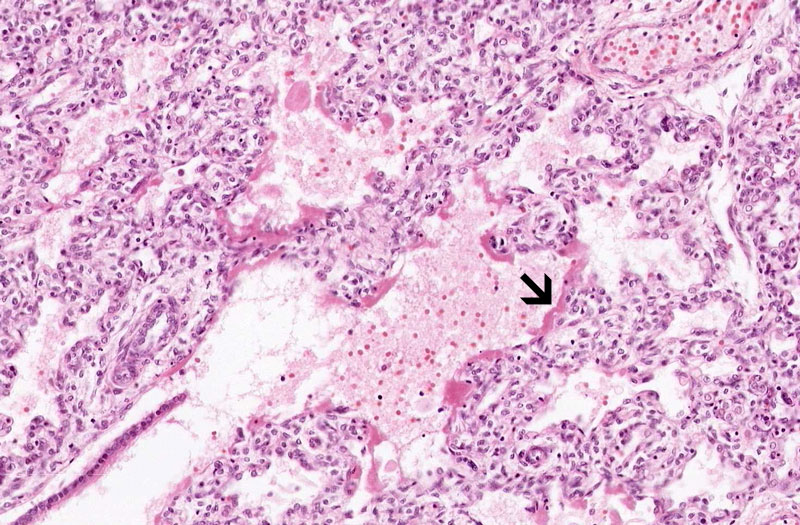
What organ is this?
From the histologic perspectives for medical students, the first
goal is to identify the organ of this slide. At the scanning level,
it looks partially solid but there are some small slits in between.
There are also some tubule like structures (arrow). On a closer
look, these tubules are lined by ciliated columnar epithelium and
some may have cartilage next to it and these are
bronchi/bronchioles. On higher magnification, you can appreciate
that the solid looking areas are in fact immature pulmonary alveoli
that has not fully expanded which end up giving this kind of solid
look at low magnification. The alveolar space can be clearly
recognized.
-
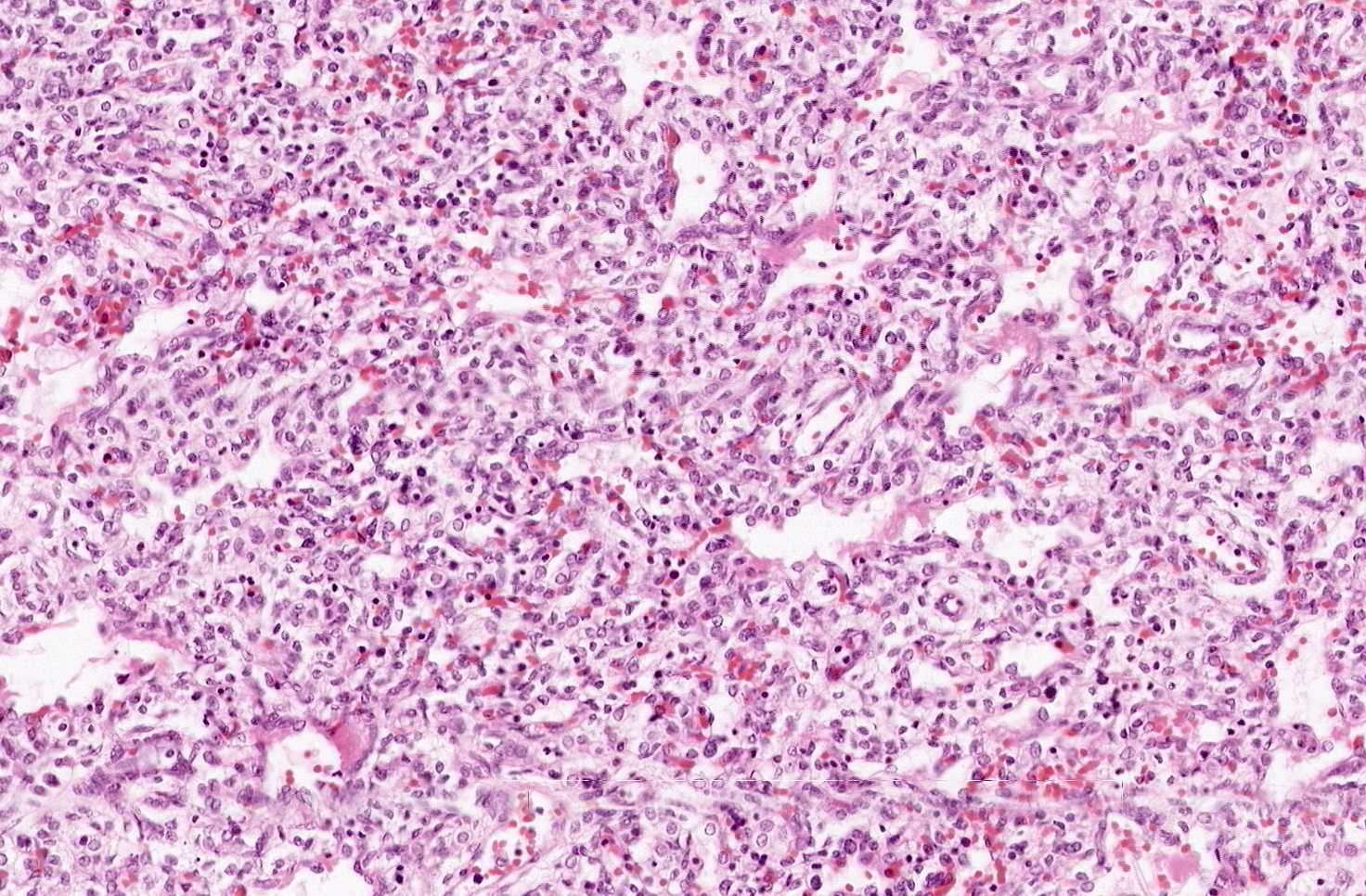
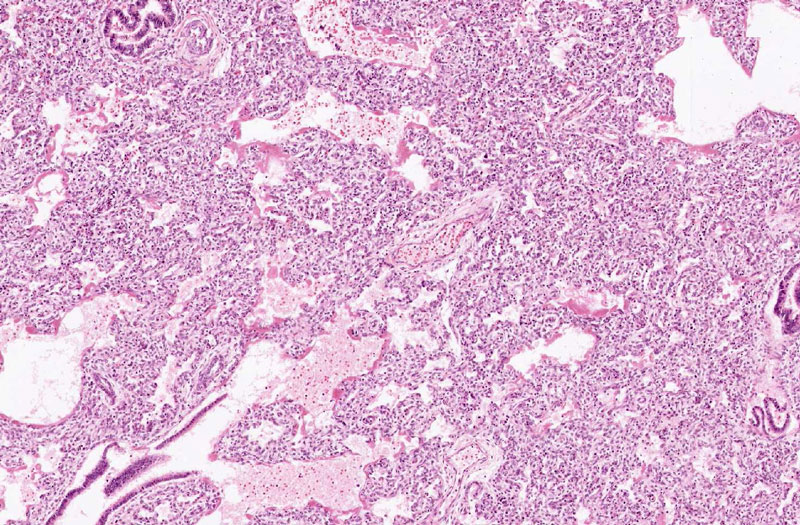
In general, there is no inflammatory cell infiltration and the
alveolar spaces are only partially expanded or not expanded at all.
-
Although the alveolar spaces are not completely expanded, distal
airways and proximal air spaces (alveolar ducts) are usually dilated
and lined by a thin layer of delicate, pale eosinophilic, amorphous
transuduate-like substance known as hyaline membrane. The
hyaline membrane may form within 30 minutes after birth.
-
Lymphatics in interlobular septa are often dilated and prominent.
Edematous fluid and sometimes hemorrhage (not in this case) can be
seen.
-
Developmental malformations may co-exist but is not part of hyaline
membrane disease and therefore deserves a separate recognition.
|