Case No.: N-010
Diagnosis: Leigh's disease (Subacute necrotizing encephalopathy)
Organ: Brain
Last Updated: 12/31/2009
|
|
|
Hematoxylin & eosin |
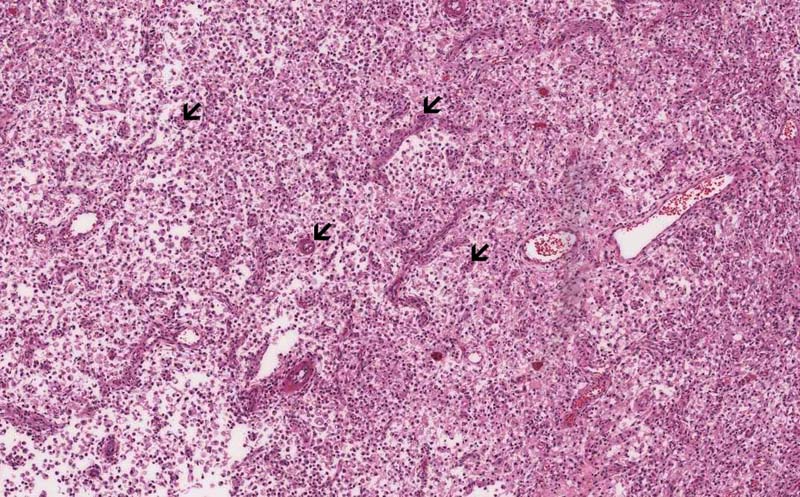
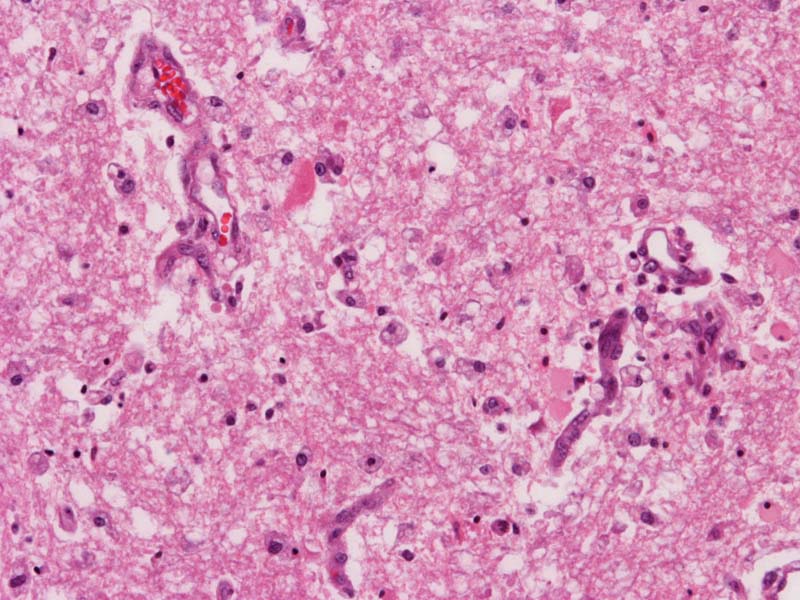
Area 1: The necrotic area is characterized by seas of foamy histiocytes with increased number of blood vessels (arrows). |
|
Hematoxylin & eosin |
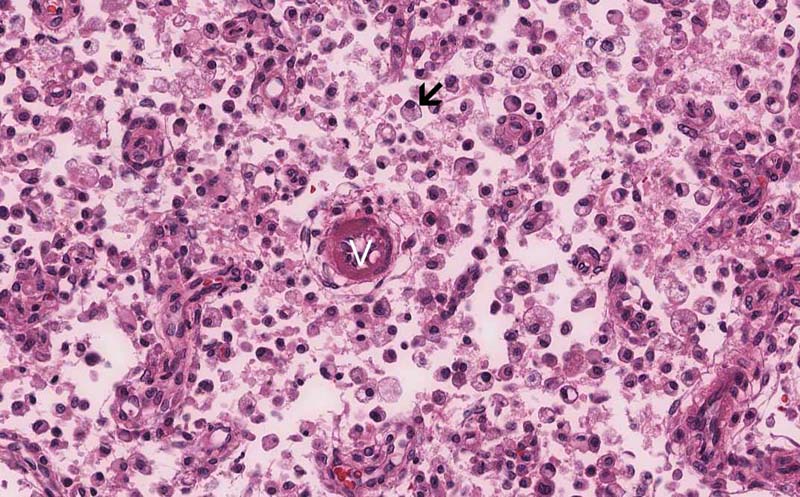
Area 1: The foamy histiocytes (macrphages) acquire the foamy morphology by having a substantial amount of lysosomes in the cytoplasm which make these cells foamy in appearance (arrow). Many blood vessels (V) are also present. |
|
Hematoxylin & eosin |
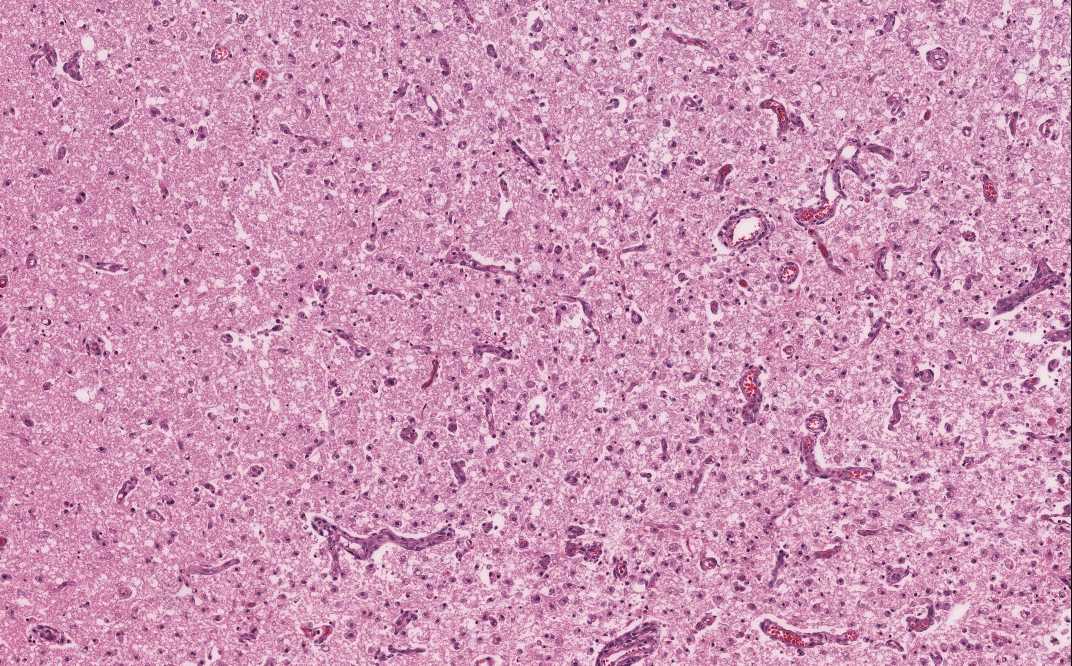
Area 2: This image is taken from an area that is less necrotic and the tissue is more intact. There is an increase in the number of blood vessels in these relatively intact areas, a feature of Leigh's disease. If you magnify this area in the online slides, you can also see foamy histiocytes even though they are not as numerous as those in the frankly necrotic areas. |
|
History: The deceased was a 7 month-old girl who was born by spontaneous vaginal delivery and his course was unremarakble for the first three months of life. Her neurological status then deteriorate rapidly. Manifestations include loss of developmental mile stones, hypotonia, recurrent vomiting, and seizure. MRI scan demonstrated multiple lesions in the cerebral hemispheres which affect mainly the deep gray matter and also the gray matter of the brain stem as well as spinal gray matter. She died at the age of 7 months.
Gross Pathology: The deep gray matter (thalamus and basal ganglia) demonstrate necrosis that involves symmetrical areas which involves mainly the gray matter (large arrows). Similar lesions are also present in the brainstem and cerebellum (small arrows). In all of these areas, there is disintegration of tissue. No hemorrhage is noted. The mammillary bodies are relative unaffected. The area with substantia is extensively necrotic. [Click here to see the gross photos again]
Histologic Highlights of this Case:
General Information:
|
Bonus Images:
|
Hematoxylin & eosin |
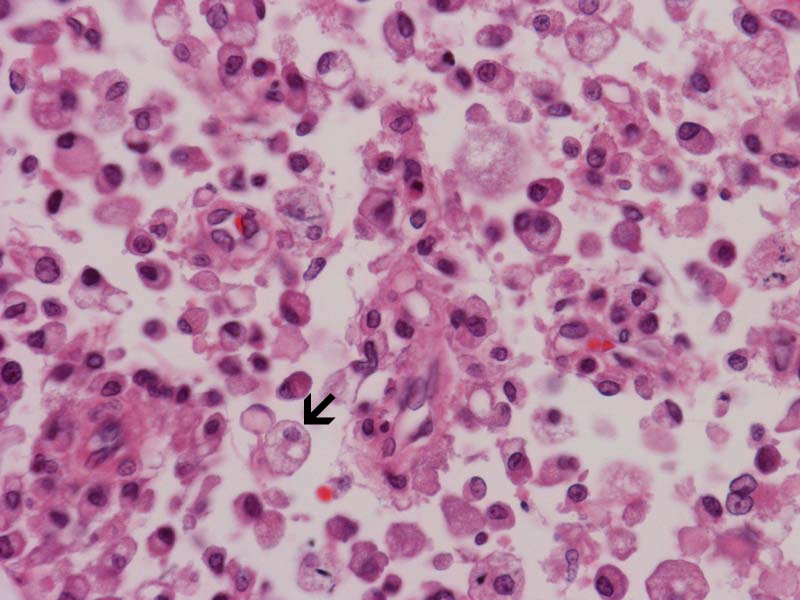
High-magnification image on the histiocytes: The foamy histology is best illustrated in this high-magnification image. |
|
Hematoxylin & eosin |
Relatively unaffected area: This high-magnification image is taken from the relatively unaffected area similar to Area 2. Note the foamy histiocytes. |
|
|
CD163: The distribution of the foamy histiocytes corresponds to the necrotic areas and is best illustrated in this online slides. CD163 is a commonly used immunohistochemistry for macrophages. |
|
|
Neurofilament proteins: Immunohistochemistry for neurofilament proteins identify the areas that are relative spared from the necrosis where axons (containing neurofilament proteins) are spared. These areas corresponds to areas with less macrophages found. Compare this online slides with the one with immunohistochemistry for CD163. |
|
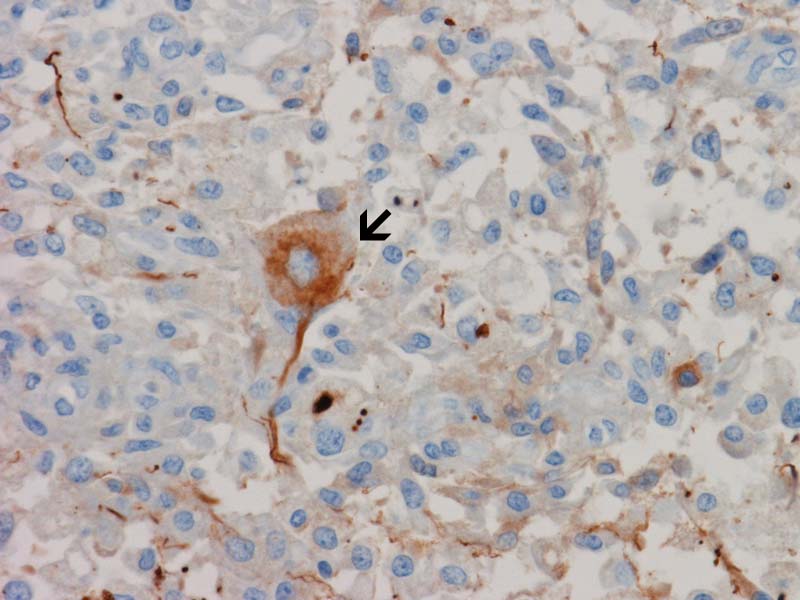
Neurofilament |
Spared neurons: One of the characteristics of Leigh's disease is relative preservation of neurons in the necrotic areas. These neurons may not be easy to be found on hematoxylin and eosin stain but they can be demonstrated easily by immunohistochemistry for neurofilament proteins as in this case (arrow). Note that the surrounding histiocytes are negative for neurofilament proteins. |
|
|
Glia;l fibrillary acidic protein (GFAP): A substantial amount of reactive gliosis is present and is best illustrated by immunohistochemisty for GFAP as illustrated by this online image. |
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.