Case No.: N-015
Diagnosis: Gliosarcoma with rhabdoid changes
Organ: Brain, cerebral hemisphere
Last Updated: 08/21/2010
|
|
|
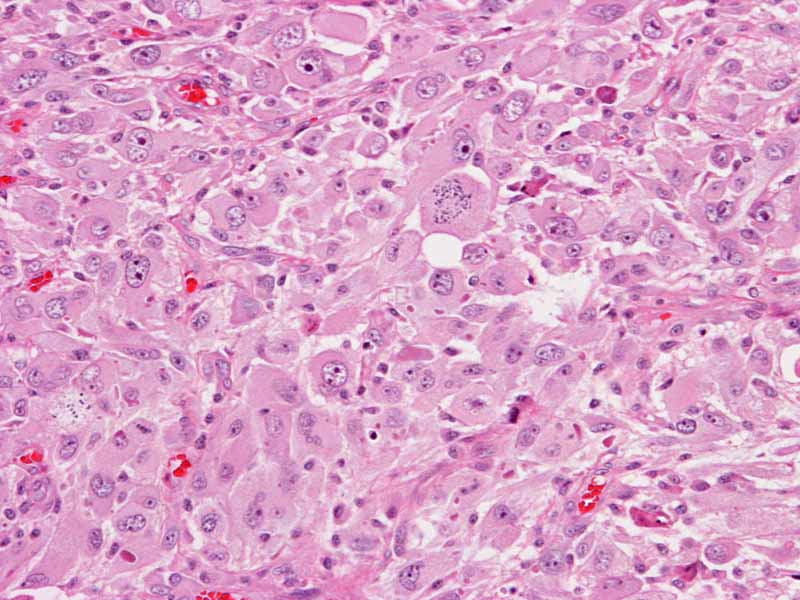
Hematoxylin & eosin |
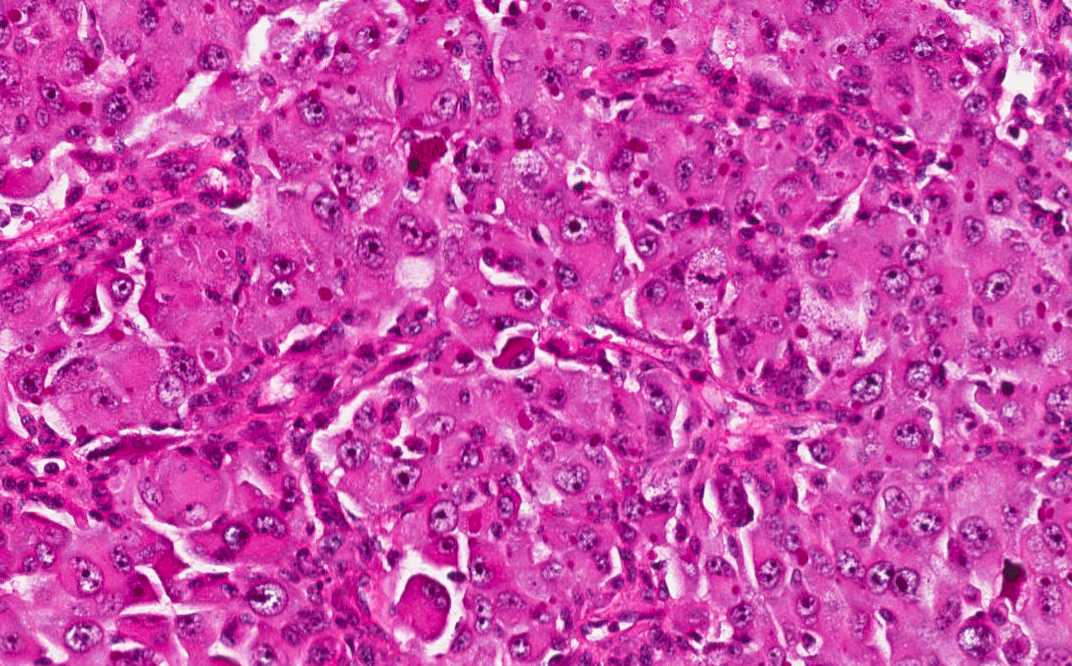
Area 1: The tumor is composed of large, pleomorphic cells with large nucleoli. The tumor cells are densely packed and without any pattern formation. The nuclei are large and there are prominent nucleoli. A moderate amount of cytoplasm is also present. The morphology varies from more spindle appearing to more epithelioid appearing. |
|
Hematoxylin & eosin |
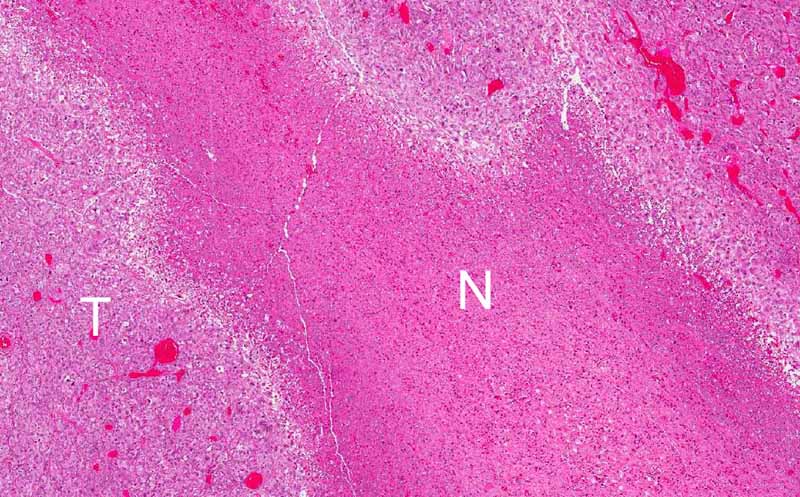
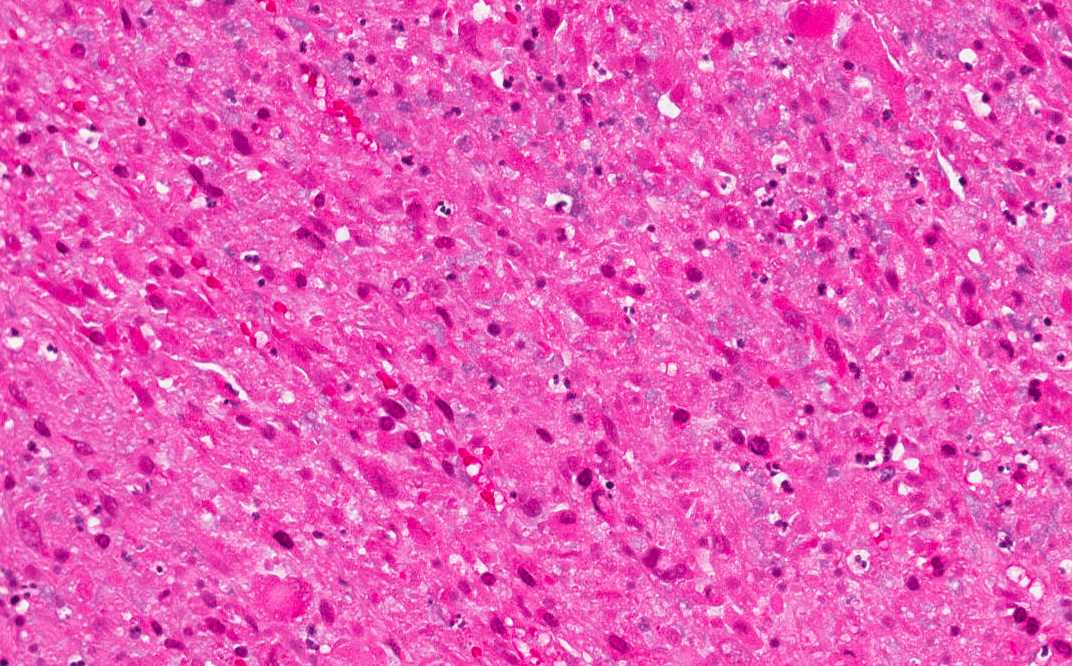
Area 2: Geographic areas of necrosis (N) is present in this tumor (T). Note that no pseudopalisading necrosis, one of the salient features of glioblastoma, is not see here. Compare the necrotic area in high magnification with that of the viable tumor cells. Note the loss of cellular details. |
|
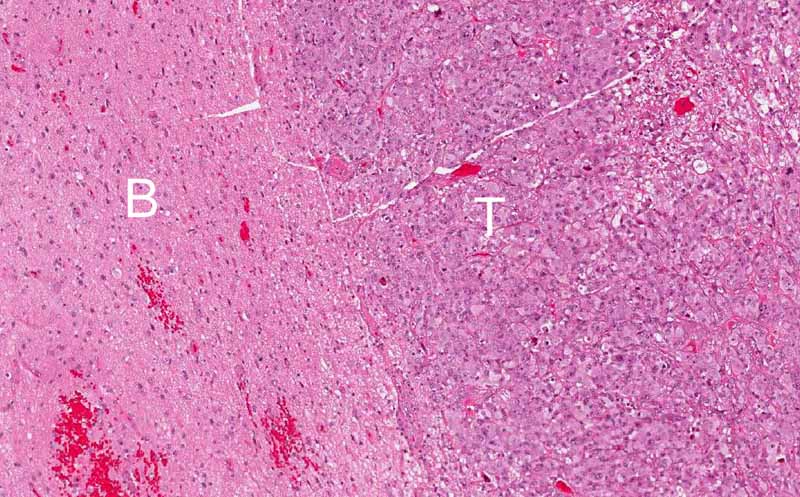
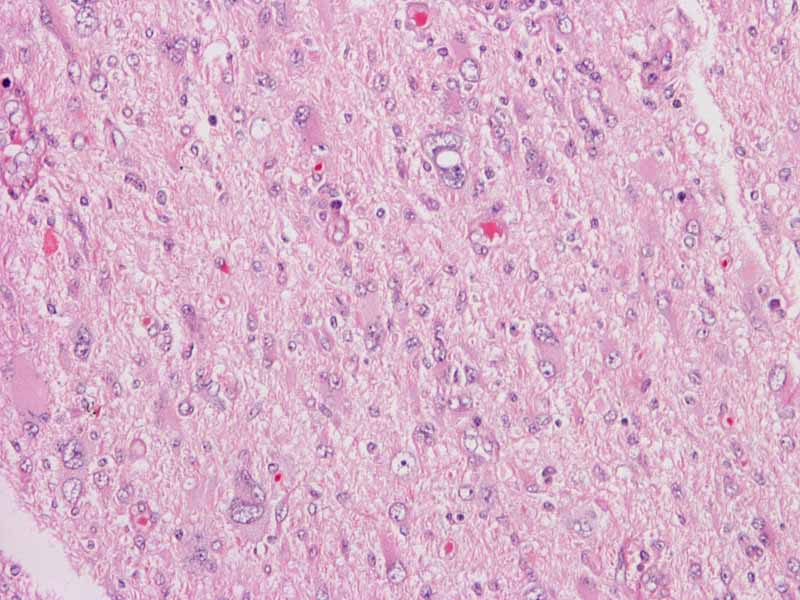
Hematoxylin & eosin |
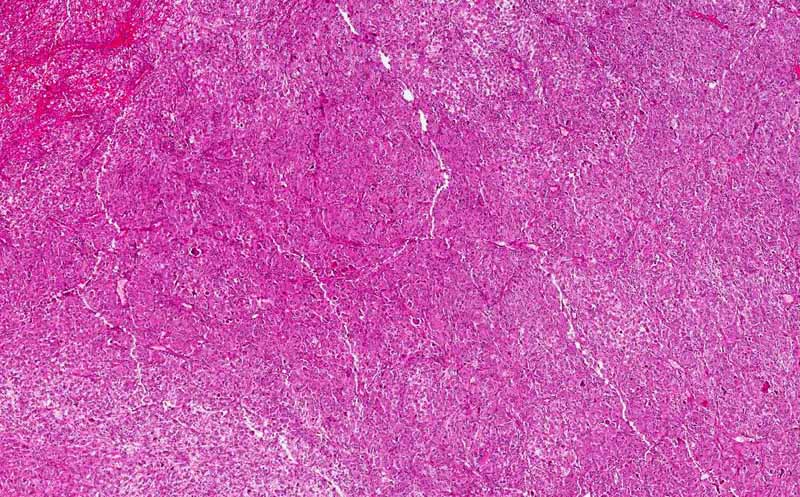
Area 3: The tumor (T) is overall very well demarcated from the surrounding brain tissue (B). This is also an unusual feature of glioblastoma or anaplastic astrocytoma which usually have an infiltrative margin. This features also explain why the tumor appears well demaracted enough to suggest meningioma on imaging studies. |
|
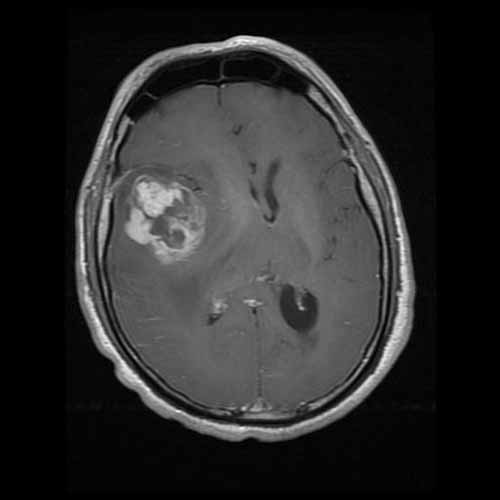
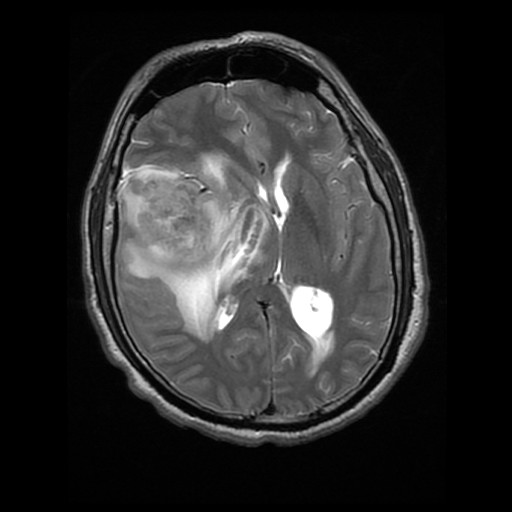
History: The patient was a 43 year-old man who complained of a 4 week long history of nausea, vomiting, and headache with pain in the central forehead area. He reported also a 6 day long severe pain and dizziness so severe that he could not leave home. His neurological examination was free from focal signs or weakness. An MRI scan demonstrated an avidly enhancing mass, 5.2 x 4.4 x 4.9 cm, in the right frontal parietal area that was most likely extra-axial and with dural tail enhancement. There is substantial edema around the mass as demonstrated on FLAIR images. The mass was excised and yielded the specimen being shown here.
MRI:
Histologic Highlights of this Case:
Immunohistochemistry:
Comment:
|
Bonus Images:
|
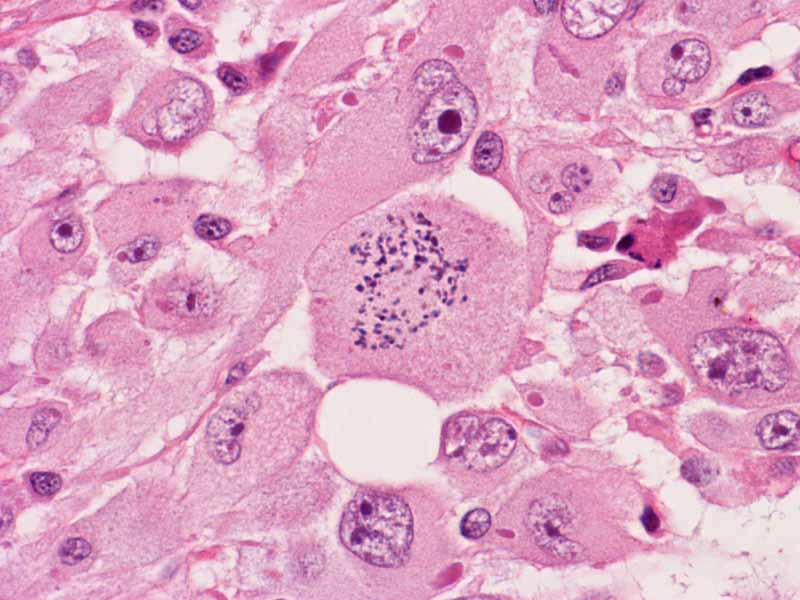
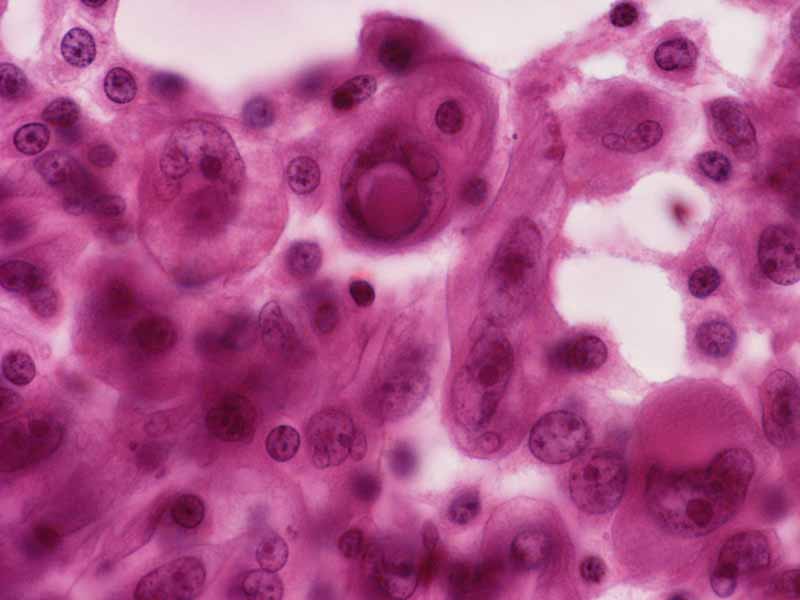
Hematoxylin & eosin |
This image is taken from another slide of this case. In this area, the rhabdoid features are more prominent. Rhabdoid changes are featured by a large nuclei with prominent nucleoli. The cells is typically in an oval shape with a large belly of cytoplasm that pushes the nucleus to an eccentric location. Within the belly of cytoplasm is often a faintly defined inclusion body like body which may appear fibrillary on hematoxylin and eosin stain. This structure is composed largely of vimentin and will be strongly highlighted by immunohistochemistry for vimentin. |
|
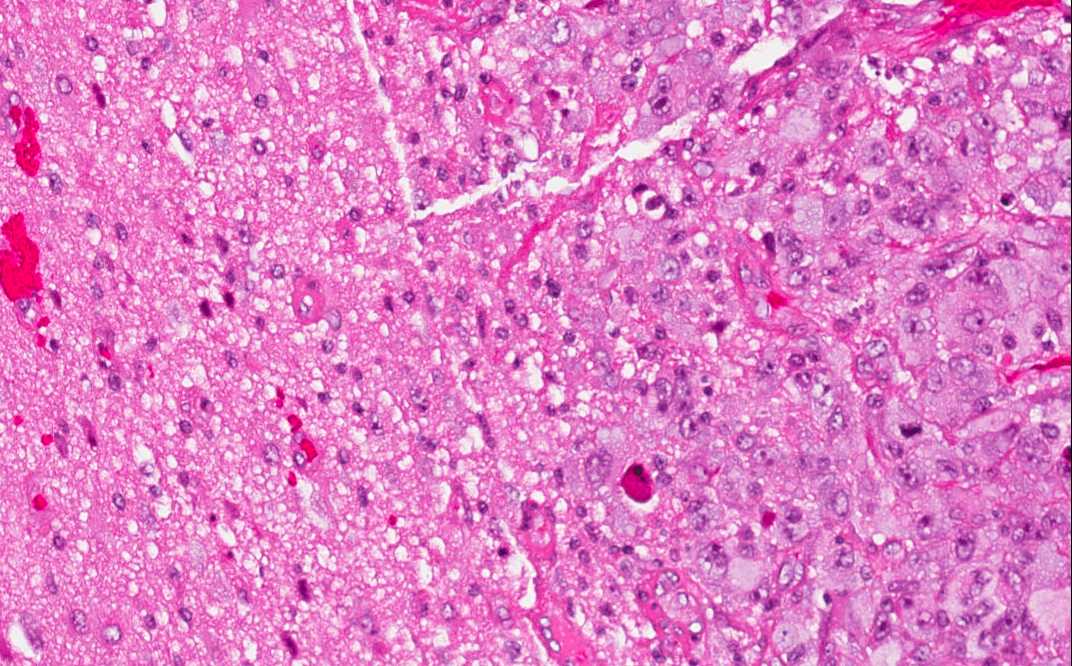
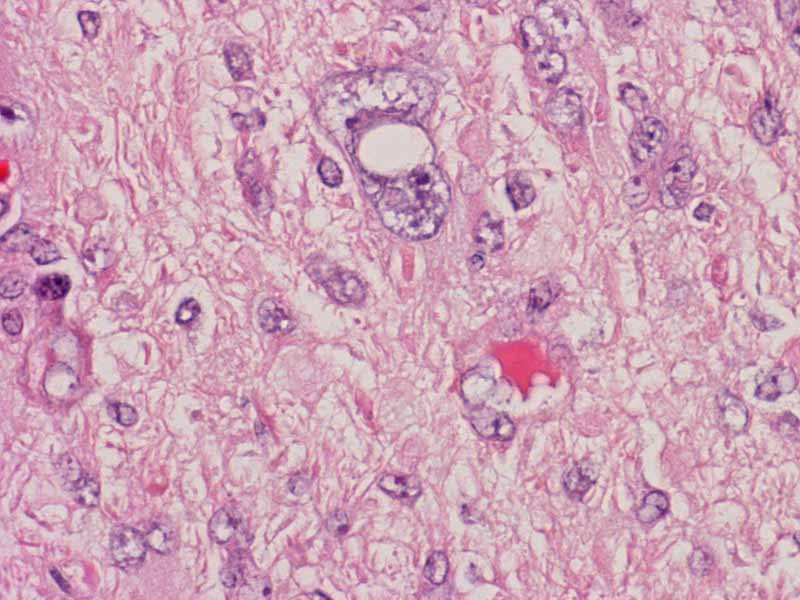
Hematoxylin & eosin |
This image is taken from another slide of this case at the interface between the tumor and the brain tissue. Note that the infiltrating tumor cells. Compare this area with Area 3. |
|
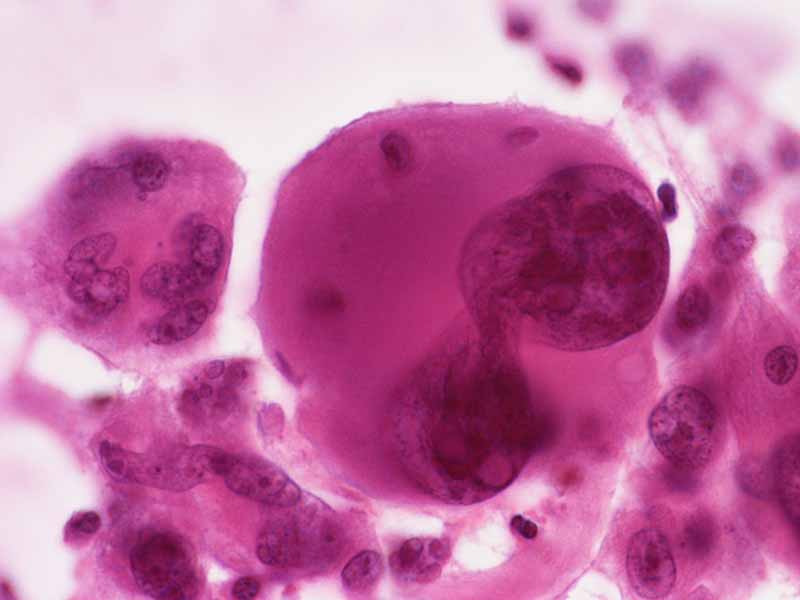
Hematoxylin & eosin |
This image is taken from the cytologic prepartion of this case at the time of intraoperative consultation. The rhabdoid features are well shown here. Many multinucleated tumor giant cells are present. |
|
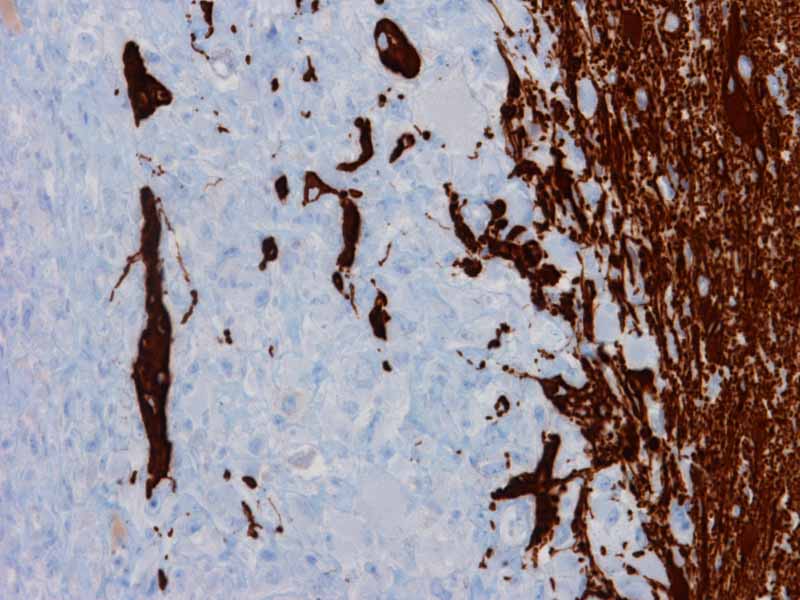
Glail fibrillary acidic protein (GFAP) |
Glial fibrillary acidic protein (GFAP): Focal but strong immunopositivity is present in this tumor. |
|
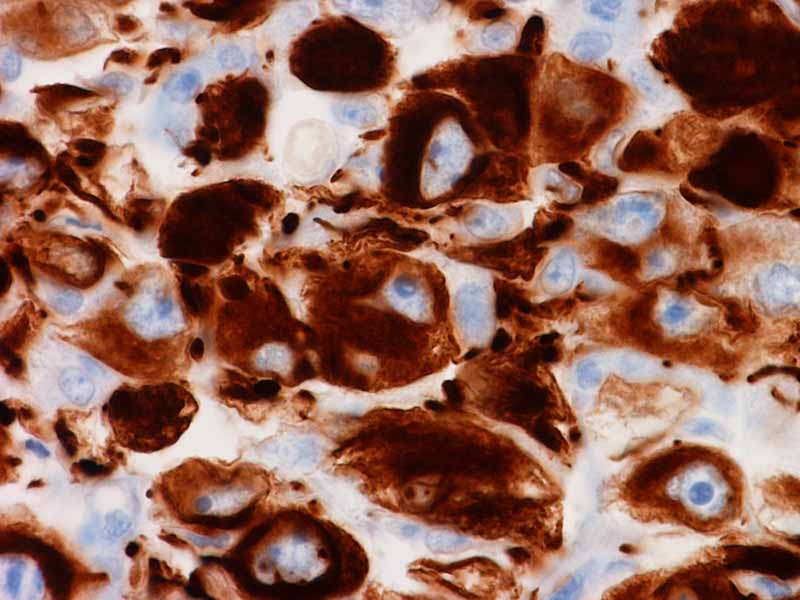
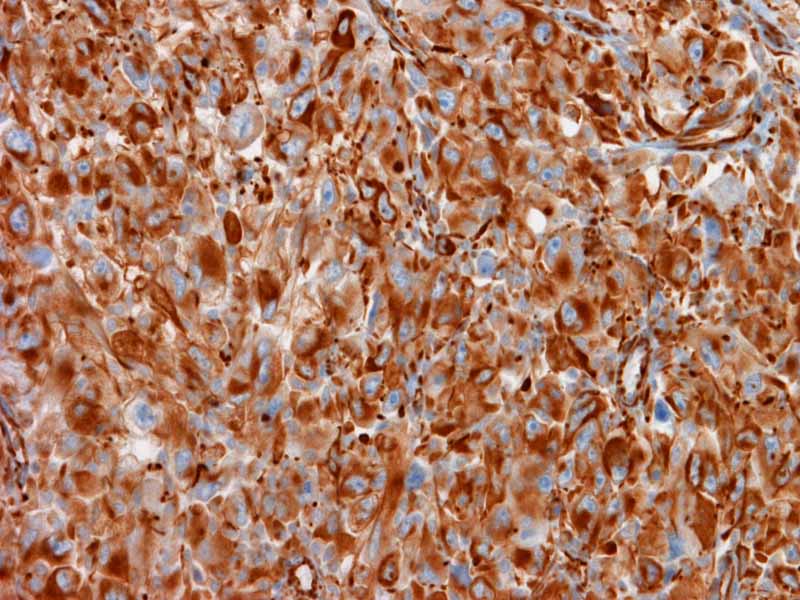
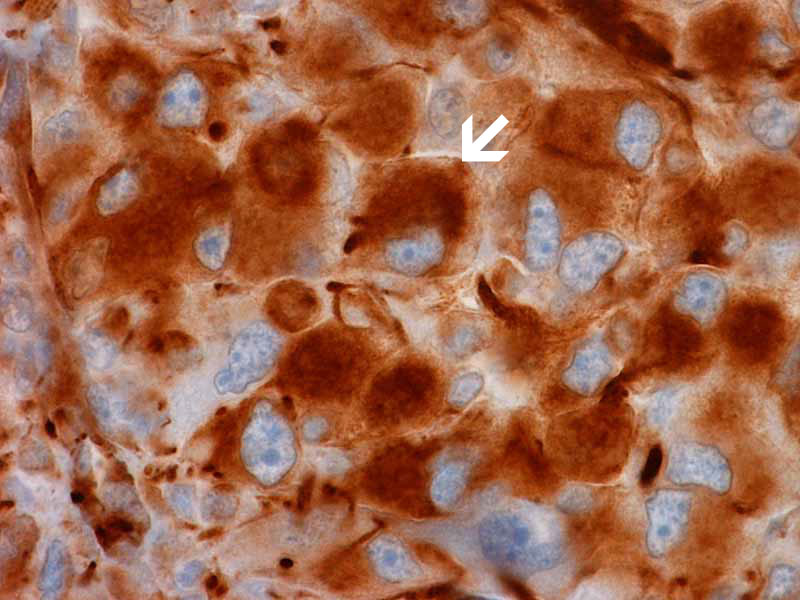
Vimentin |
Vimentin: Practically every cell is immunoreactive for vimentin. Note the belly of strongly positive cytoplasm in the tumor cells. This feature is rather characteristic for rhabdoid cells. |
|
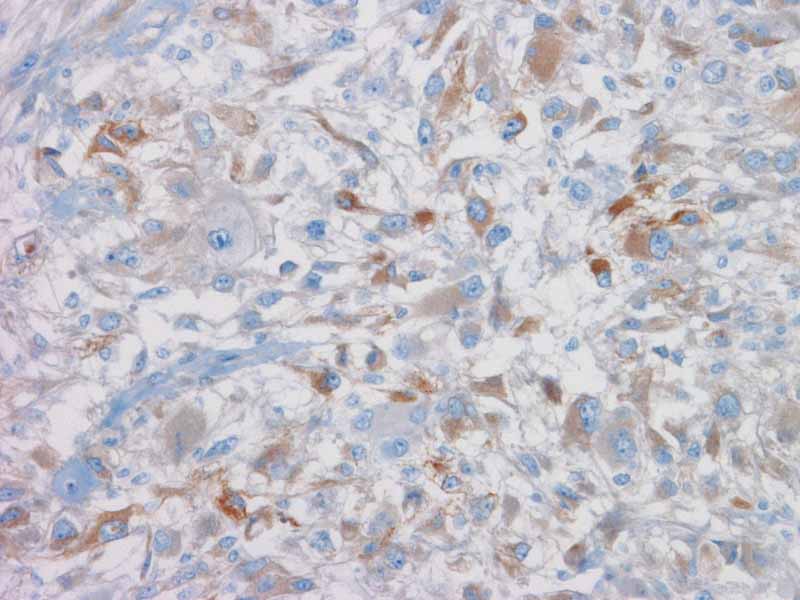
Epithelial membrane antigen (EMA) |
Epithelial membrane antigen (EMA): Only weak and very focal immunoreactivity is noted. |
|
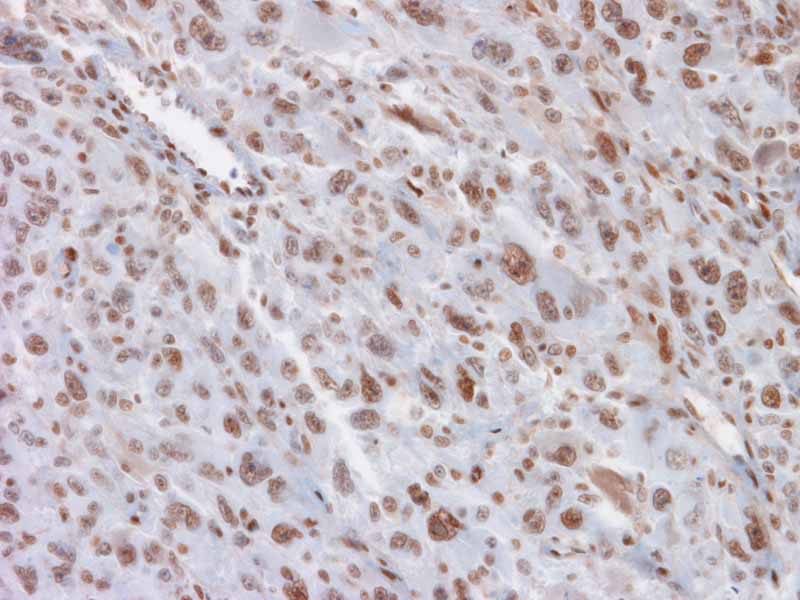
BAF47 |
BAF47: Positive immunoreactivity is present. This antibody stains for the gene product of INI1 gene which is deleted or mutated in ATRT. When the gene is deleted or mutated, the immunoreactivity will be lost. The preservation of immunoreactivity indicates that the gene is not deleted and most likely not mutated. |
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.