Case No.: N-018
Diagnosis: Atypical teratoid rhabdoid tumor (ATRT)
Organ: Brain, ventricular-thalamic mass, left side
Last Updated: 09/21/2010
|
|
|
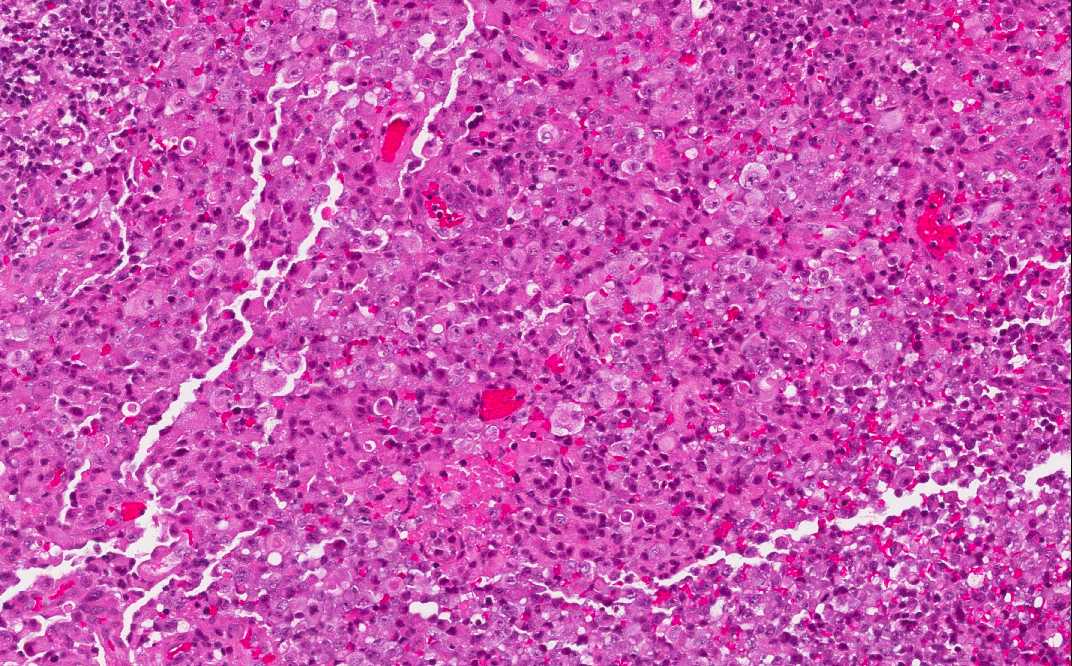
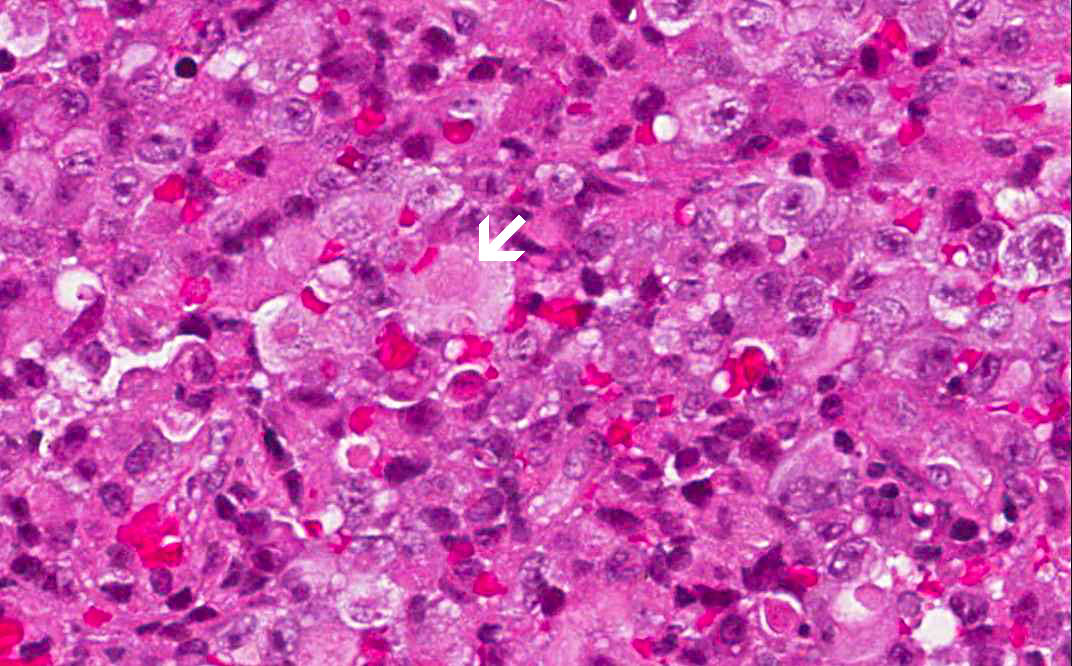
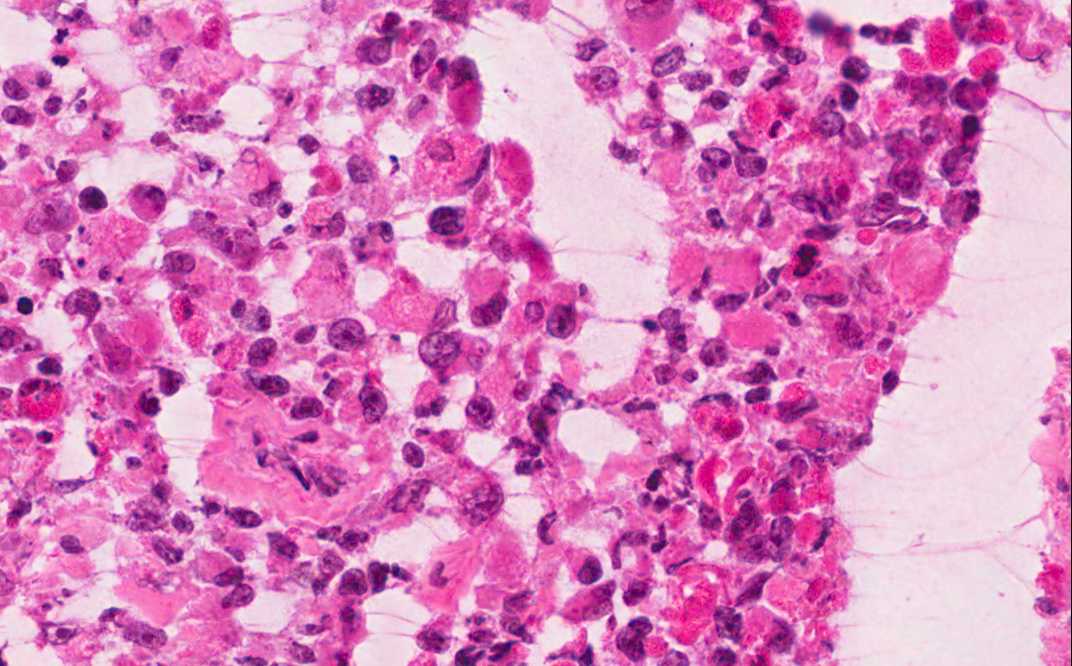
Hematoxylin & eosin |
Area 1: The tumor is solidly packed with round to oval cells of comparable size but there is a definitive variation of cellular size. The nuclei are large and have prominent nucleoli. The larger cells have amphophilic cytoplasm and eccentrically located nuclei. In some of the tumor cells, there is a centrally located round inclusion-like, poorly demarcated fibrillary substance that is more dense looking than the surrounding cytoplasm. These inclusion-like bodies are typically contains a substantial amount of vimentin and would be strongly positive for vimentin. |
|
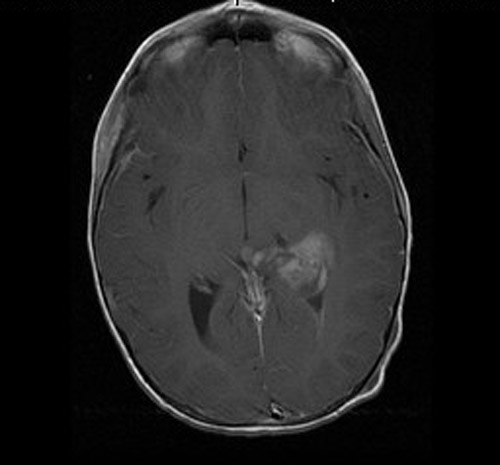
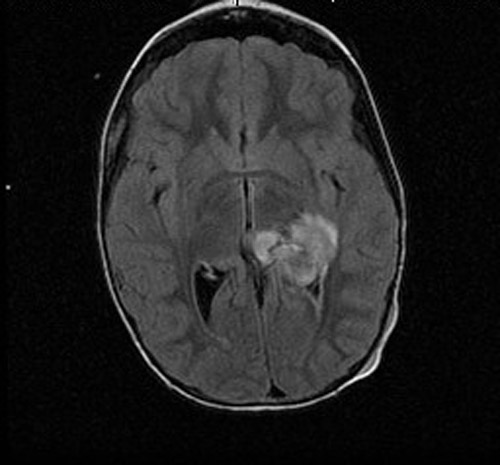
History: The patient was a 6 year-old girl who presented with a history of Streptococcal infection about 3 weeks ago and was treated with Amoxicillin. She improved briefly but started vomiting, hip pain, neck pain, and severe headache. She was treated with antibiotics under the impression of meningitis and she improved again. However, she started vomiting for several times again and was admitted to the emergency. An MRI scan demonstrated a brain mass as illustrated here. The lesion was excised and yielded this specimen.
Imaging Studies:
Histologic Highlights of this Case:
Comment:
|
Bonus Images:
|
BAF-47 |
Immunohistochemistry for BAF-47: This antibody detects the gene product of INI1 gene. When this gene is intact, the nuclei will stain positive. When it is deleted or mutated, the gene nuclei will not contain the protein and therefore stained negative. Therefore, negative staining indicates positive deletion or mutation of INI1 gene. Endothelial cells are typically positive which may serve as an internal positive control. In this case, there are some tumor cells that are positive. It is the unpublished experience of the author (KMF) that cases with heterozygous deletion of chromosome 22q tends to have some weak positive immunoreactivity in a small number of tumor cells. |
|
Hematoxylin & eosin |
Intraoperative cytologic operation: The rhaboid cells are best detected in the cytologic preparations. |
|
Hematoxylin & eosin |
Intraoperative frozen section: The rhabdoid features of the tumor cells are readily seen at the time of intraoperative crozen section. This part of the specimen has more necrosis than the part submitted for permanent section. |
Original slide is contributed by Dr. Kar-Ming
Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.
Home Page