Case No.: N-019 Quiz
Diagnosis: Diffuse astrocytoma, WHO grade II
Organ: Brain, frontal-temporal region
Last Updated: 12/21/2010
|
|
 Hematoxylin & eosin |
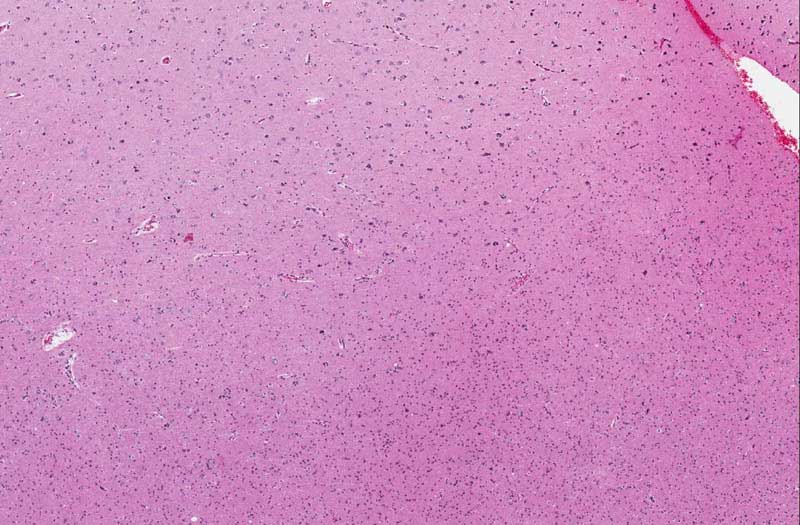
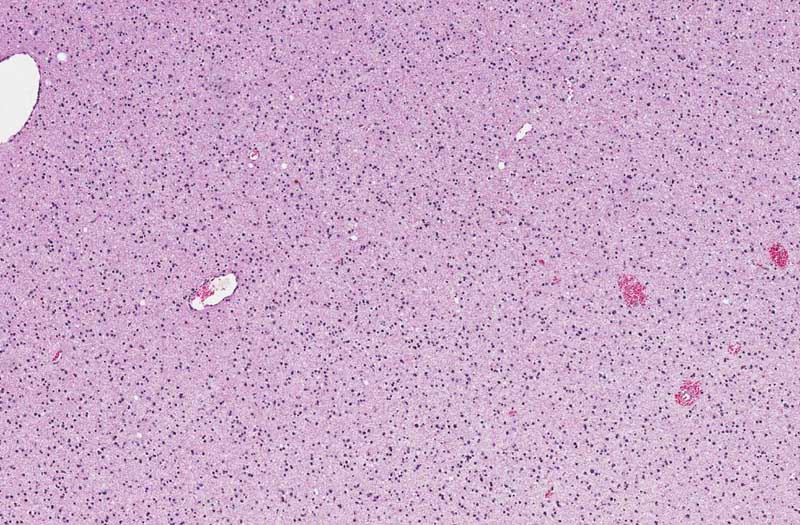
Area 1: The cellularity (the number of cells per unit area) in the deep white matter is increased. The cytoplasmic processes are rather coarse and in between the processes are some bluish mucoid material. These material are very classic for low grade glial neoplasm. Microcysts are often a common feature of low grade glial neoplasms although they are not present here. These cysts often contain this type of mucoid material. |
|
Hematoxylin & eosin |
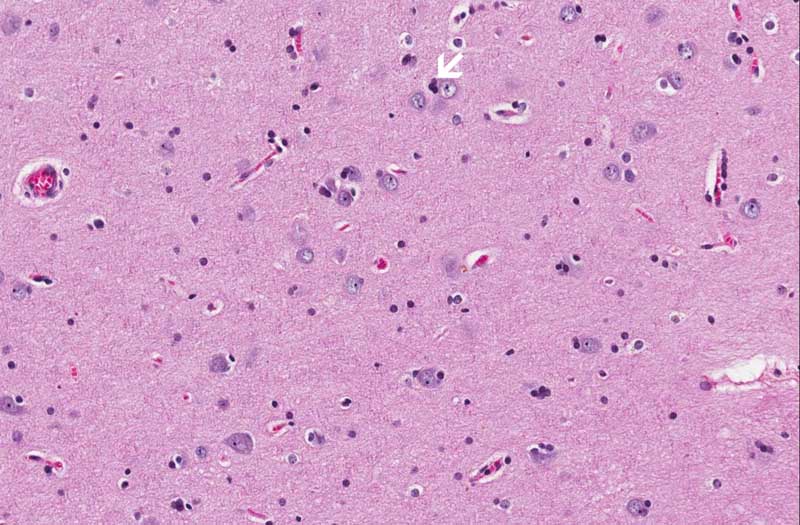
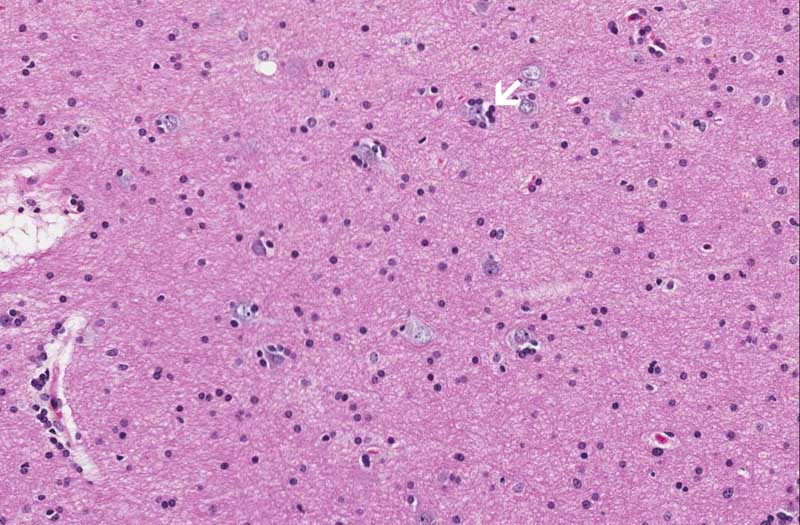
Area 2: These images are taken from an area where the cortex is infiltrated by the tumor. Image B is taken from a place more superficial (farther from the tumor) than image C which is taken from a location closer to the tumor. Note the tumor cells circling neurons (arrow) and this phenomenon is known as satellitosis (arrows in B and C). |
 Hematoxylin & eosin |
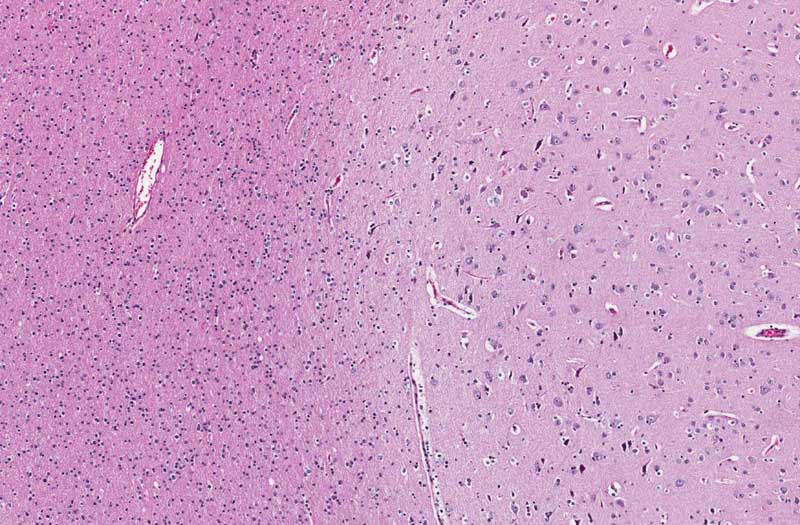
Area 3: There is still increased in cellularity in the white matter indicating the presence of tumor in this area. However, the gray-white junction is much more distinct in comparison to area 2. |
|
History: The patient was a 25 year old woman who complained of headache. MRI revealed a large, non-enhancing tumor in the frontal-temporal lobe. The mass was excised and yielded the current specimen.
Histologic Highlights of this Case:
Immunohistochemistry:
Comment:
|
Bonus Images:
|
Hematoxylin & eosin |
Luxol fast blue- Cresyl Violet |
For Comparison: This is a section taken from the parietal lobe of a patient (autopsy) with no significant histologic abnormalities. You can compare the cellularity of the white matter and the sharp gray white matter distinction with the current slide. |
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.