|
History: The patient was a 62
year-old woman with an extra-axial parasagittal mass that has been
followed by the neurosurgery clinics for some time. There was slow
increase in size and the mass was excised and yielded the current
lesion.
Imaging:
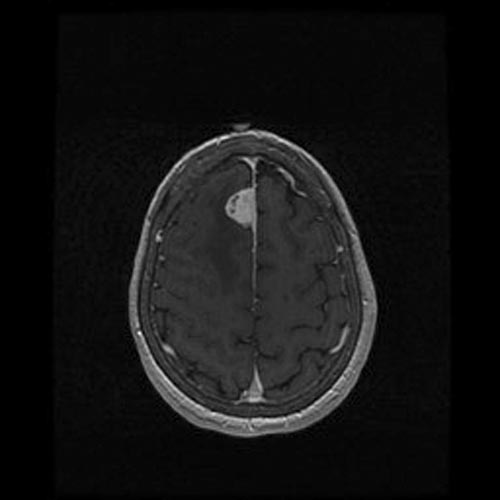
On MRI scan, there is a dural based, parafalcine mass, 2.5 cm in
greatest dimension, with vasogenic edema in the surrounding brain
parenchyma. The mass enhances brightly. There was also associated dural
thickening and enhancement along the falx.
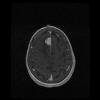
MRI T1-Contrast
Histologic Highlights of this Case:
-
The received specimen consists of rather
rubbery fragments of tan, light brown tissue fragments. They are
rather cohesive and no cytologic preparation was performed at the
time of frozen section.
-
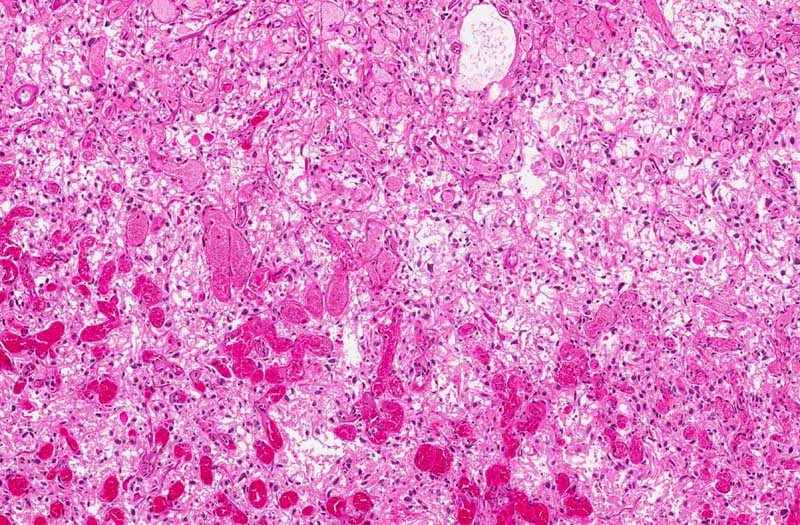
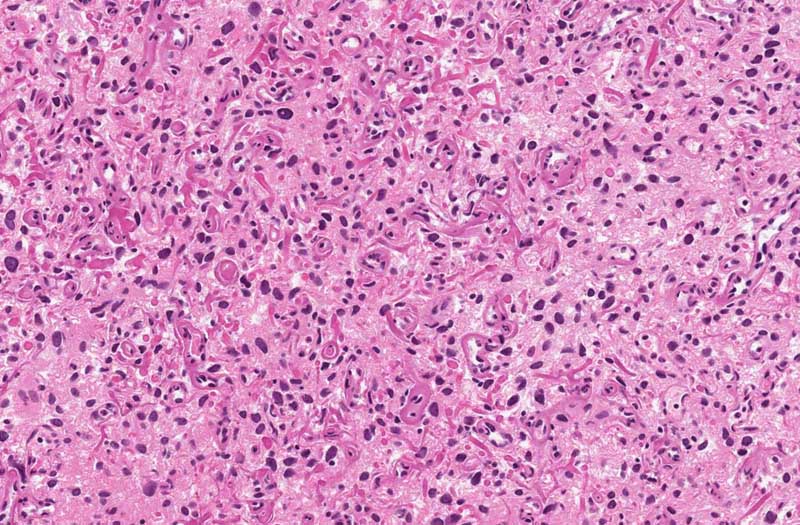
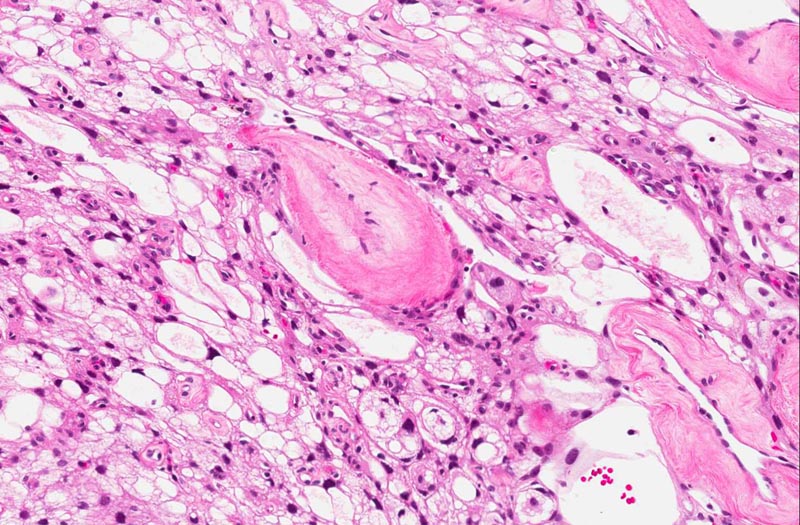
Slide #1 represent the tissue that are
received at the time of frozen. Only half of the tissue was
submitted for frozen and the slide being shown here represents the
portion that have not been frozen. This specimen appears to be a
highly vascular lesion with quite a good amount of stromal cells in
between (area 1 and 2). Note that the stromal cells have
hyperchromatic nuclei but no prominent nucleoli. There are no
intranuclear inclusions or high grade pleomorphism. No definitive
clear cells were observed. Definitive sclerotic changes are present
in many of the blood vessels.
-
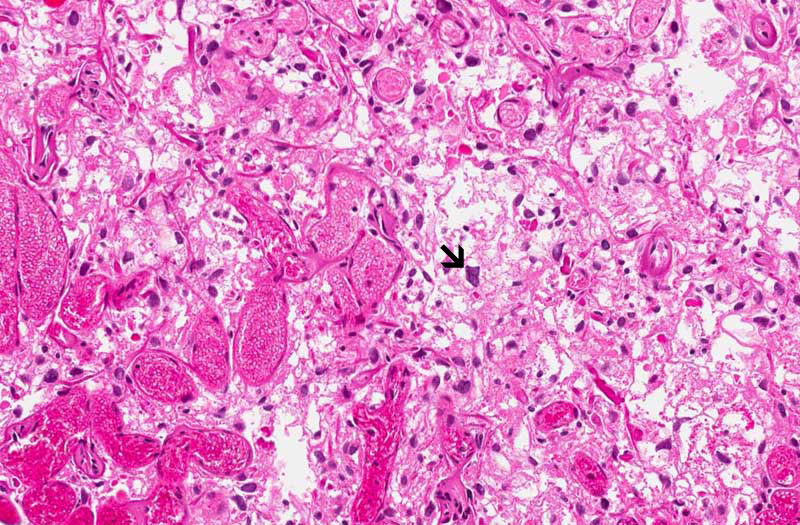
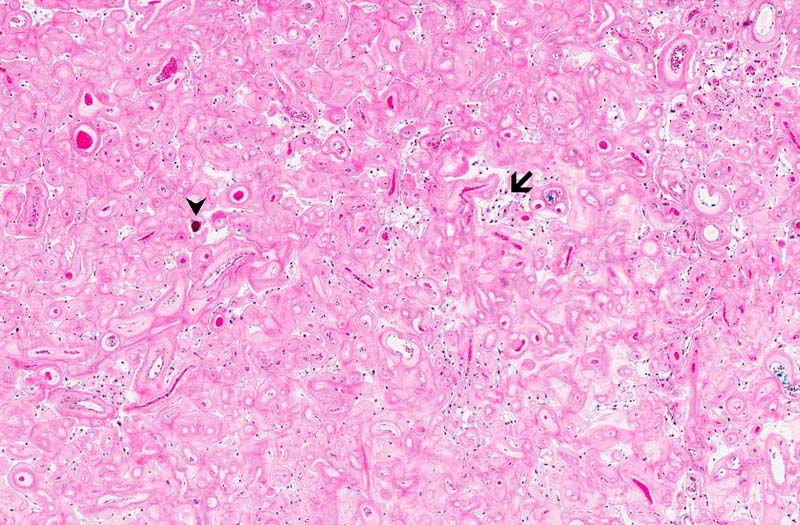
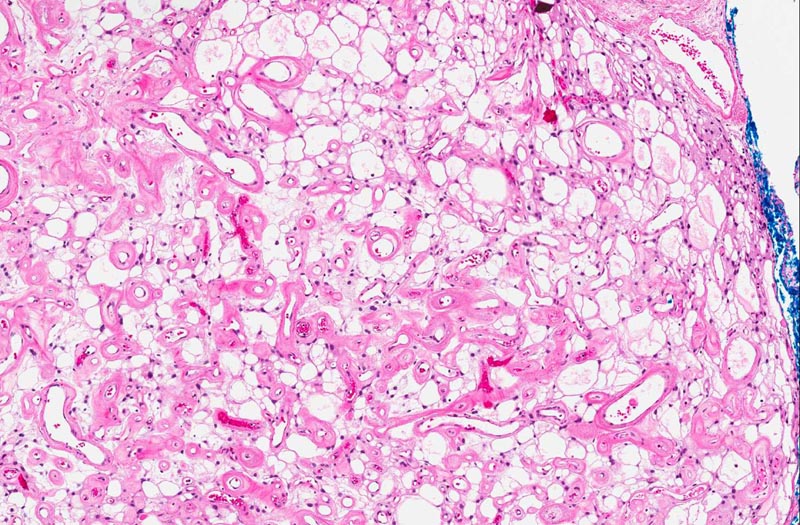
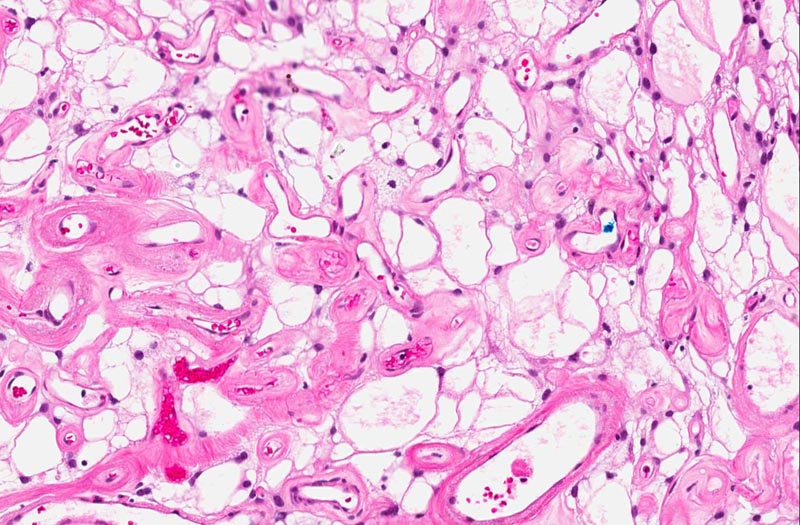
Slide #2 represent the tissue that are
submitted subsequently. The histopathology between this sample and
slide #1 is essentially similar but the there are a lot more highly
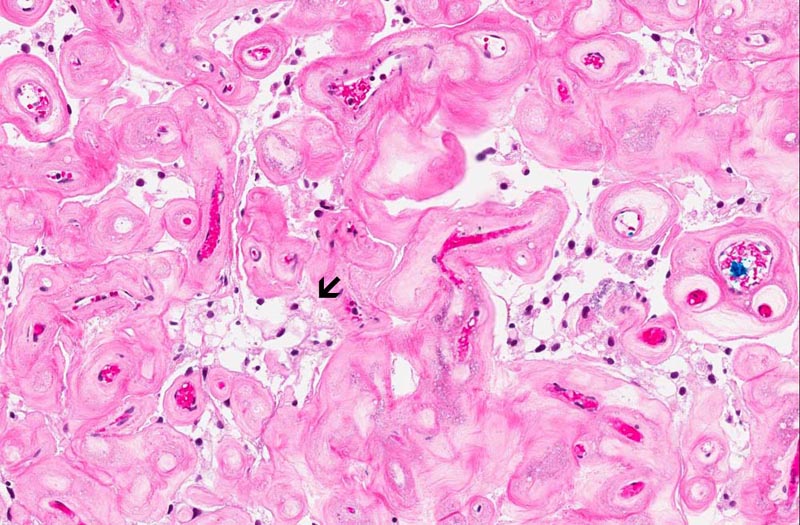
sclerotic blood vessels. Some calcifications consistent with
psammoma bodies are present (area 3). The sclerotic blood vessels
dominated the picture. In between the sclerotic vessels are
triangular to irregular nest of stromal cells (area 3). Microcyst
formation is rather common (area 4 and 5).
-
Mitotic figures are not readily seen.
Histopathology:
-
Cytokeratin: Negative in all components.
-
Inhibit: Negative in all components.
-
Epithelial membrane antigen (EMA):
Negative in all components.
-
Glut1: Positive in endothelial cells and
stromal cell component.
-
CD31: Positive in endothelial cells and
negative in stromal cells.
-
CD34: Positive in endothelial cells and
negative in stromal cells.
Discussion:
-
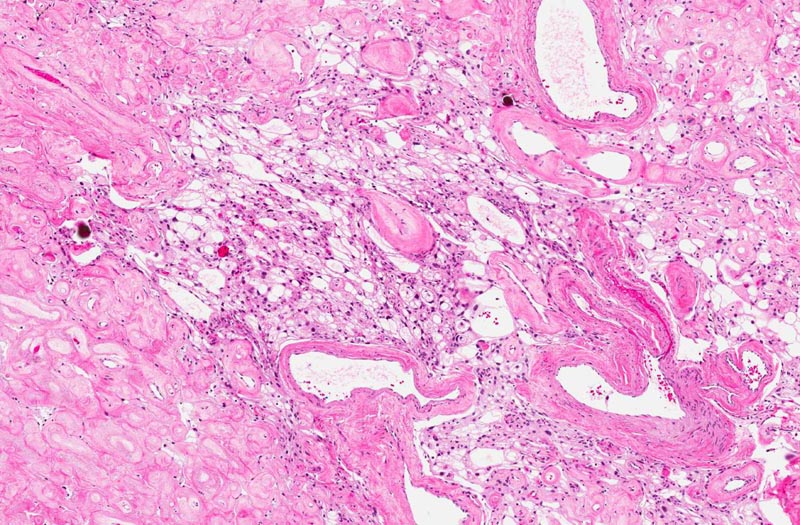
The overall histopathologic picture is
that of an angiomatous meningioma. These tumor are featured by
hypervascularity and often with degenerative changes of the vessels
including vascular hyalinization as illustrated in this case. The
nuclei tends to undergo degenerative atypia (ancient changes)
featured by slightly enlarged, homogeneously hyperchormatic nuclei
without prominent nucleoli and not associated with increased
mitosis. The neoplastic meningothelial proliferation often has microcystic
pattern as illustrated here.
-
EMA is often but not always
positive in meningioma and it is negative in this case. A lack of
immuoreactivity for EMA does not rule out a diagnosis of meningioma.
One of the possibile explanation for the lack of EMA
immunoreactivity in this case is that EMA immunoreactivity is often
patchy in meningioma. The total volume of meningothelial
proliferation is not that much in this case and the bulk of the
tumor is either blood vessels or empty spaces in the microcysts.
-
The main differential diagnosis of this
case is hemangioblastoma. Slide #1 have features quite suspicious of
hemangioblastoma. Cerebral hemisphere is not the most common one for
hemangioblastoma and they are not typically dural based. Their
incidence in descending order is cerebellum (80%) followed by the
medulla and spinal cord. The location and MRI findings, however, are
very typical for a meningioma. Hemangioblastoma often, but not
always, have clear cells. Their blood vessels are typically delicate
rather than hyalinized. The histologic features, particularly the
microcystic changes, degenerative atypia of nuclei, and sclerotic
blood vessels, are also in favor of angiomatous meningioma. The
psammoma bodies are also good clue for meningioma. Hemangioblastoma
is often immunoreactive for inhibin which is negative in this case.
Glut1 immunoreactivity in hemangioblastoma should be positive in
endothelial cells and negative in stromal cells.
The current case is positive in both component. The negative
immunoreactivity for cytokeratin and the overall histopathology also
rule out the possibility of a metastatic carcinoma.
|