Online Slide/Full Screen/Open with ImageScope
Case No.: N-026
Diagnosis: Meningitis in systemic coccidiodomycosis
Organ: Brain, cerebral hemispheres
Last Updated: 11/21/2011
|
|
Online Slide/Full Screen/Open with ImageScope |
|
Hematoxylin & eosin |
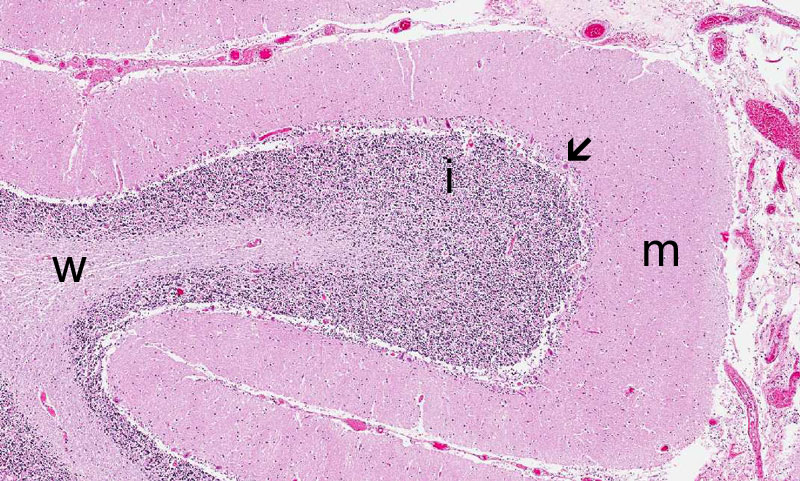
Area 1: You should be able to recognize that this is the cerebellum as the signature molecular layer (m), Purkinje cells (arrow), internal granular layer (i), and white matter (w) are present in the typical anatomical relationship. |
|
Hematoxylin & eosin |
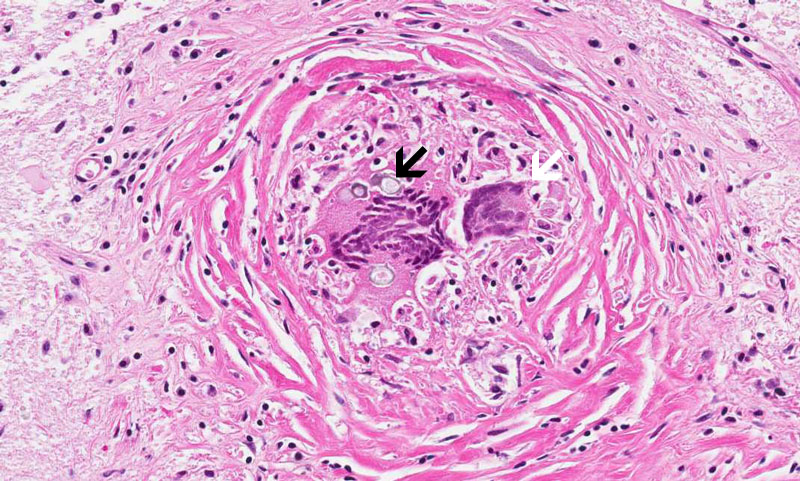
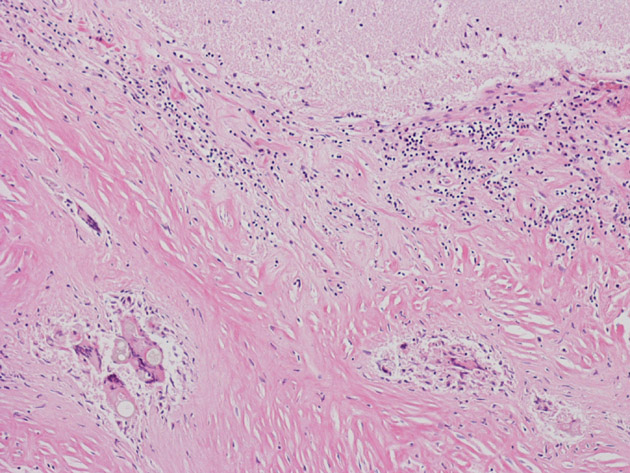
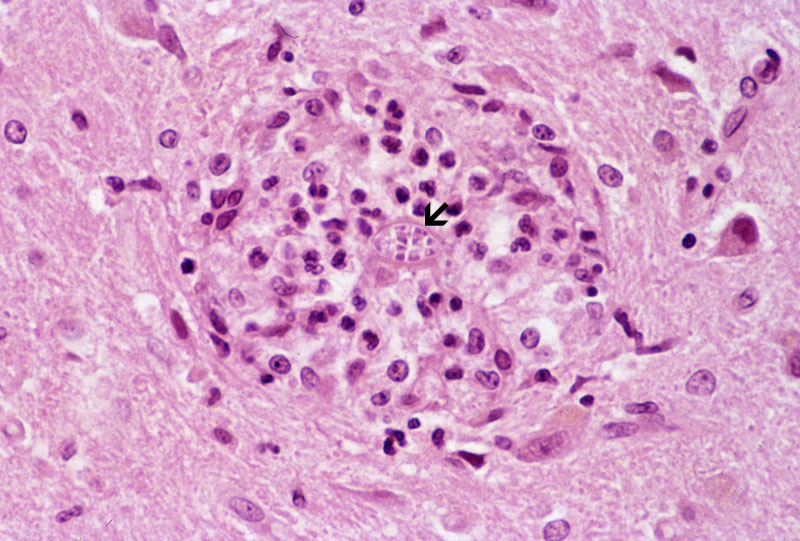
Area 2: The granulomas are composed of histiocytes in concentric arrangements forming nodules. At the center of the granulomas are mulitnucleated ginat cells containing the fungus. |
|
Hematoxylin & eosin |
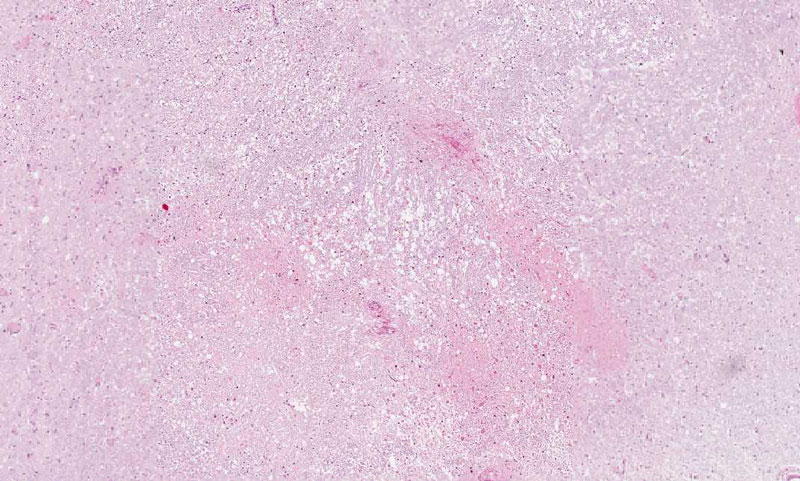
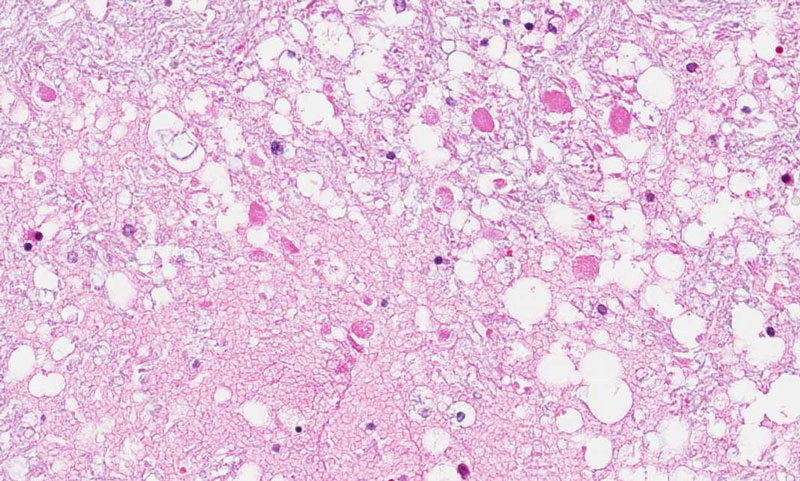
Area 3: In this area, the brain is necrotic but is not involved by the microorganism or inflammation. The reason for the necrosis is compromised circulation probably secondary to the systemic problem and the meningitis. |
|
Hematoxylin & eosin |
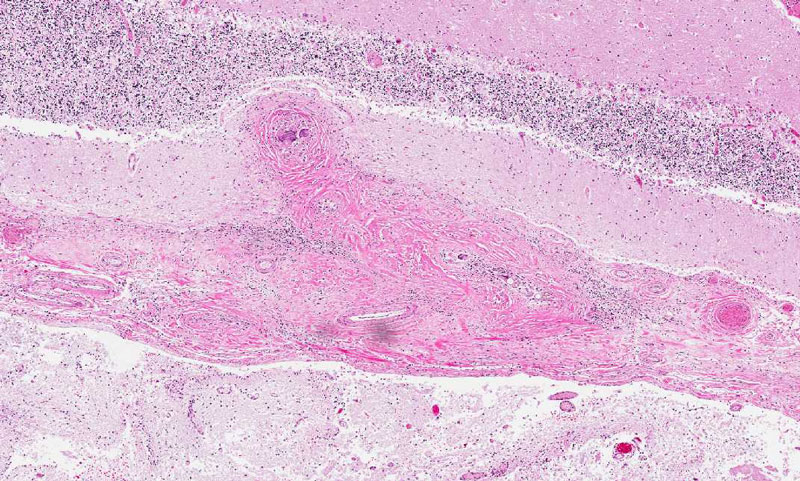
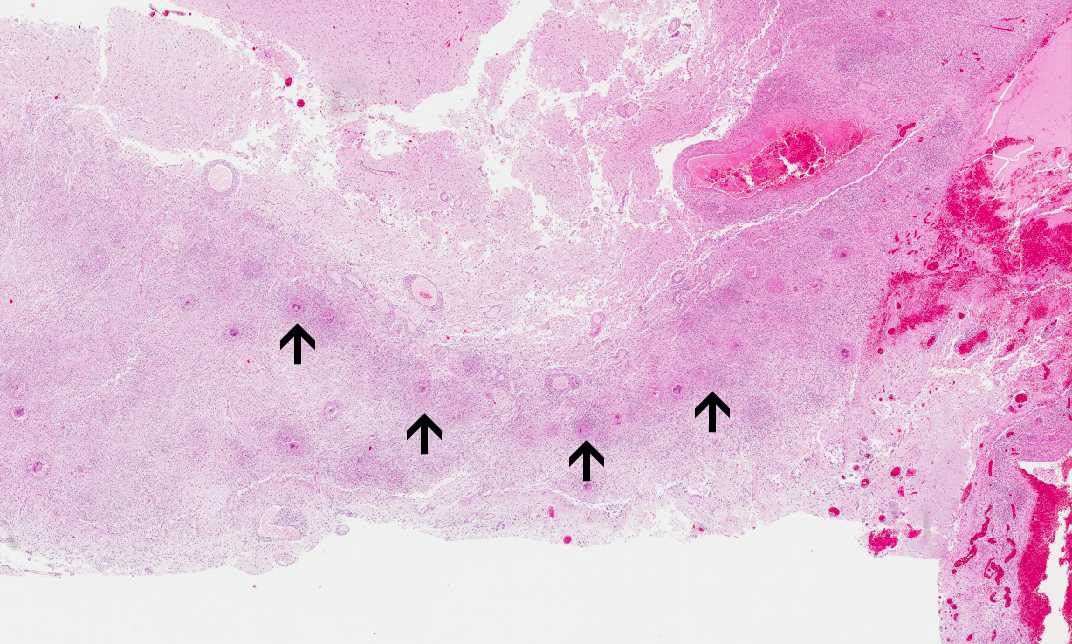
Area 4: In this image, you can see numerous granulomas (arrow) lining along the dura. |
|
History: The patient was a 20 year-old man with a history of meningitis and ventricular-peritoneal shunt placement about two years before his death. His general condition deteriorated and has multiple seizure. Despite aggressive treatment including shunt replacement, the patient expired. Autopsy was limited to the lung and the brain.
Additional History: The patient was proved to have coccidioidomycosis at the initial diagnosis of meningitis two years before his death.
Gross Pathology of the Brain: The brain weighted 1,500 grams at autopsy. It was extremely soft and fell apart on handling. The leptomeninges in the brain stem had fibrotic thickening to about 2 mm and is also firmly attached to the brain parenchyma. The dura is also significantly thickened.
Pathology of the lung: Similar pathologic changes were seen in both the lung and the brain.
Histologic Highlights of this Case:
Comment:
|
Bonus Images:
|
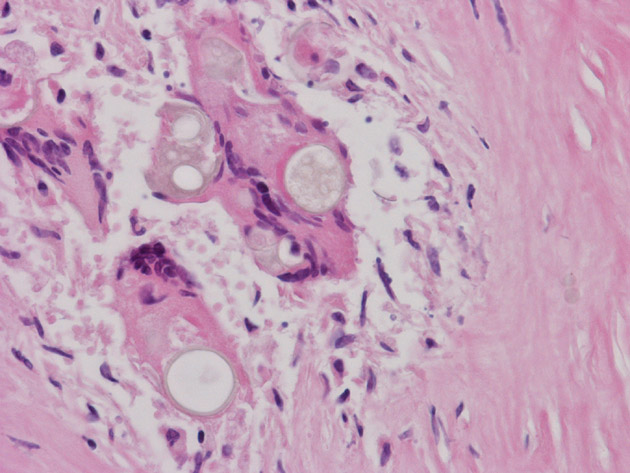
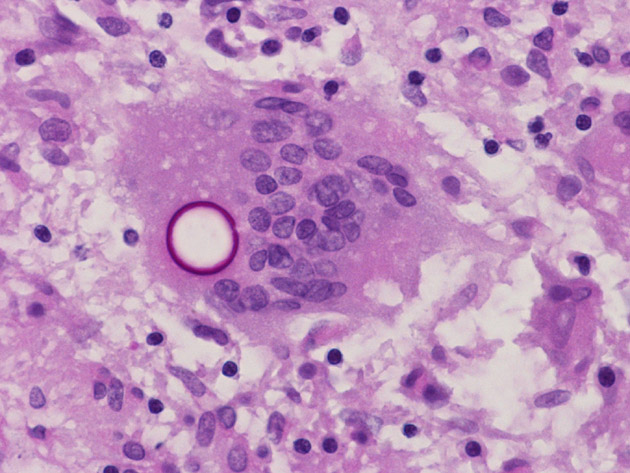
Hematoxylin & eosin |
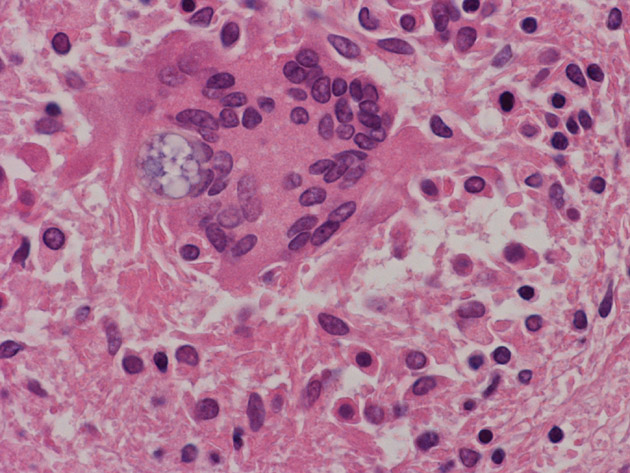
High magnification HE stain image: Note that the fungal organisms do not take up the stain and remains either as a pale, round clear structure or with some bluish content. |
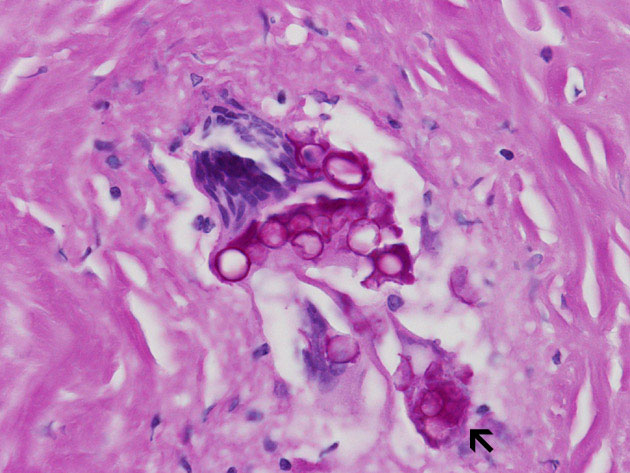
 PAS stain |
High magnification PAS stain image: In contrast, the outline of cell wall can be well highlighted by periodic acid Schiff (PAS) stain as illustrated in these images. In this case, most of the fungal organisms do not contain viable endospores which may be resulted from prolonged antifungal therapy. However, one of the funcal organisms containing spores may be present in the PAS stain (arrow). |
|
Hematoxylin & eosin |
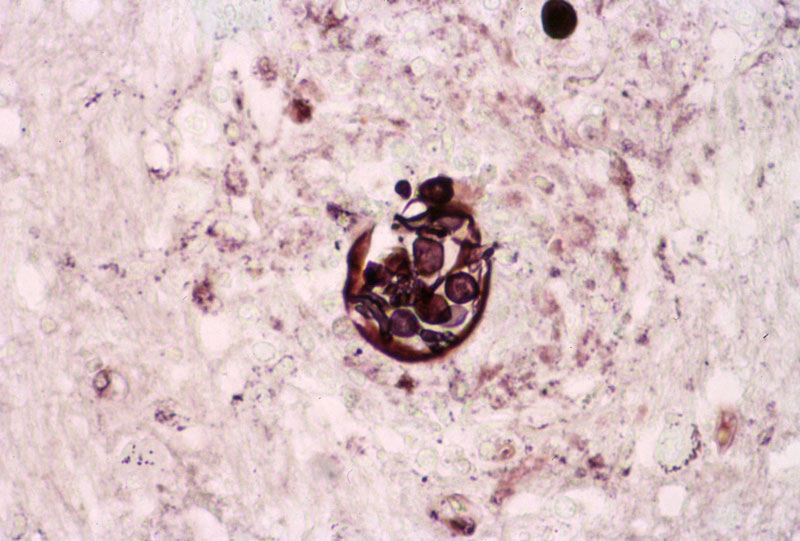
Gomori's methanamine silver (GMS) |
Image from another case: In this case of infection of the brain parenchyma, the small spores within a spheres can be well see on hematoxylin and eosin stain (arrow) and are well demonstrated by GMS stain. Note that there is also no giant cell reaction in this case. |
Original slide is contributed by Dr. Kar-Ming Fung, University of Oklahoma Health Sciences Center, Oklahoma, U.S.A.