


| A 76 year-old Man with a Mass at the Base of
Tongue. January, 2012, Case 1201-1. Home Page |
Lewis Hassell, M.D., Cheng Z. Liu, M.D. Ph.D., Kar-Ming Fung, M.D., Ph. D.. Last update: December 31st, 2012.
Department of Pathology, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma.
Clinical information:
The patient was a 76 year-old man. He was referred from an outside hospital because of a large mass at the base of his tongue obstructing the airway and also with complain of difficulties in swallowing. A well circumscribed pedunculated mass was demonstrated by CT scan. A fine needle aspiration was performed and the mass was excised in our institute.
|
|
|
|
|
|
| A. Scanned slide | B. | C. | D. |
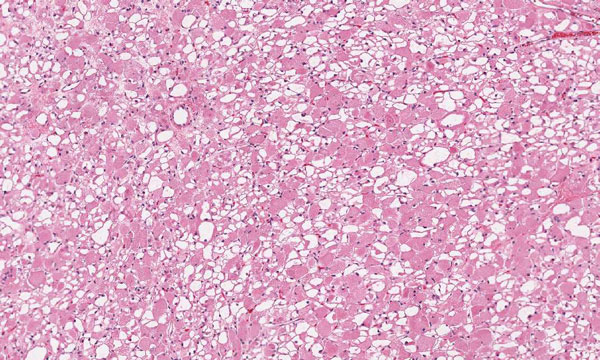
The tumor was a well circumscribed 6.0 x 3.5 x 2.0 cm and had a solid cut surface without significant hemorrhage. No necrosis was noted. The followings are representative images from this mass
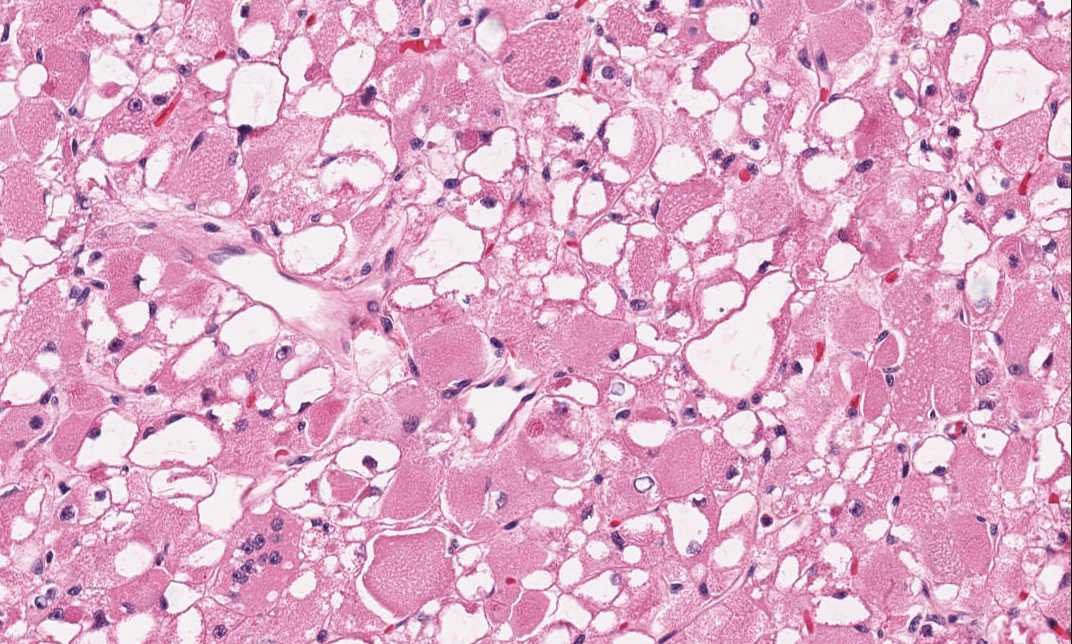
Pathology of the Case: Different parts of the tumor have rather homogeneous appearance (Panel A) which reflect the solid, homogeneous cut surface on gross pathology. Neither necrosis nor hemorrhage are present. On medium magnification, the tumor is composed of large, polygonal cells with distinct cell borders (Panel B) and eccentrically located, small, bland nuclei. The tumor cells are separated by thin fibrous septa with delicate blood vessels. Many of the cells have solid, amphophilic to slightly eosinophilic cytoplasm and other cells have large, clear cytoplasmic vacuoles. These two types of cells arranged in a checkboard type of arrangement. Small amount of brightly eosinophilic, crystalloid like substances are in the cytoplasm of cells with solid cytoplasm (arrow in Panel C). Occasional cells have centrally located nuclei and there are multiple peripheral vacuoles which makes the cytoplasm reminiscent of a spider (arrow in Panel D). These cells are known as "spider cells". Muscle striations are not conspicuous in this case.
Results of immunohistochemistry and special stain are as follow:
Immunohistochemistry:
Muscle specific actin: Positive in tumor cells.
Smooth muscle actin: Positive in tumor cells.
Desmin and myogenin: Negative in tumor cells.
Vimentin: Negative in tumor cells.
CD68: Negative in tumor cells.
PGP9.5: Negative in tumor cells.
S100 protein: Negative in tumor cells.
Cytokeratins : Negative in tumor cells
Epithelial membrane antigen: Negative in tumor cells.
Special stain:
Periodic Acid Schiff (PAS): Negative in tumor cells
PAS with diastase: Negative in tumor cells
| DIAGNOSIS: Adult rhabdomyoma |
Discussion: General Information Pathology Differential diagnosis
Adult rhabdomyoma is a benign tumor. These tumors have rather characteristic histology among different tumors and it is easy to be recognized. Arriving at a correct diagnosis is usually not a problem. What makes this case challenging is that rhabdomyoma is rare. Except for conspicuous striations, this tumor has all the signature of a rhabdomyoma including large polygonal cells with solid cytoplasm and large cytoplasmic vacuoles, cytoplasmic crystalline eosinophilic bodies which correspond to Z-disc substance at ultrastructural level, and "spider cells". This tumor is also positive for muscle specific actin. Although most rhabdomyoma are positive for desmin, the current tumor is negative for desmin.
Rhabdomyoma can be separated into the cardiac type and the extracardiac type. The extracardiac type can be further separated into the adult type, fetal type, and genital type. Adult rhabdomyoma can be seen in all ages but these tumors are most common in adults older than 40 years old and they are three times more common in male 1. Occasional cases are seen in children 2. Adult rhabdomyoma are most frequently seen in the head and neck area 1, 2, 3, 4, 5, 6, 7, 8, 9 and rare cases occurring in mediastinum 10, 11 and other locations have also been reported. Although most cases are solitary tumors, multifocal cases can occur 1, 12, 13 and the tumors are found within the head and neck area. Clinically, they are painless mass with a slow growth rate. Incidental findings during autopsy can occur. As may of them are found in the larynx and base of tongue, obstruction of the airway and difficulty in swallowing are common manifestations.
Grossly, these benign tumors are in centimeter range and have well circumscribed pushing margins. It can occur as a pedunculated mucosal or multinodular mass. The cross section is solid and finely granular with a tan to red-brown color. Necrosis should not be seen.
As illustrated in this case, these tumors has characteristic histologic features. Adult rhabdomyomas have similar features among tumors and composed of a checker board arrangement of large polygonal cells with solid amphopilic to eosinophilic cytoplasm and cells with a large cytoplasmic vacuole. Striations reminiscent of striated muscle can be seen. Phosphotungstic acid hematoxylin (PTAH) stain may help to highlight these striations. Also present in the cytoplasms are small amoung of bright eosinophilic, rod-shaped crystalline substances and these substance probably represent Z-band (Z-disc) material. These rods are well illustrated by PTAH stain. The nuclei are small, bland and are usually eccentrically located reminiscent of mature skeletal muscle. Occasionally there are cells with centrally located nuclei with contracted cytoplasm associated with vacuoles at the periphery of the cell. The contracted cytoplasm will give a shape that vaguely suggestive of a spider and these cells are known as "spider cells".
Cytologic diagnosis by fine needle aspiration (FNA) is often performed in the head and neck area. The cytologic features are quite suggestive of granular cell tumor on cytologic aspirations. It should also be noted that a lot of the vacuoles are resulted from intracellular glycogen being removed during processing. Therefore, the vacuoles are not obvious on air dried smears. With the same token, spider cells are not always seen 14, 15,16. For these reasons and their rarity, these tumors can be misdiagnosed as granular cell tumor on FNA16.
Immunohistochemically, rhabdomyoma are positive for a panel of skeletal muscle markers including desmin (90%) and muscle specific actin (100%) 1 and other markers for skeletal muscle 17, 18, 19. The current case is positive for muscle specific actin but negative for desmin which is a little unusual. It is also important to note that and more than half of these tumors are positive for S100 1. Therefore, a tumor positive for S100 does not exclude the possibility of a rhabdomyoma. Immunohistochemistry for cytokeratin, glial fibrillary acidic protein, cytokeratin, and CD68 are negative in rhabdomyoma 1.
Differential Diagnosis:
Although the histopathology is rather characteristic, it may suggest other diagnosis particularly granular cell tumor in small specimens or fine needle aspirations. Adult rhabdomyoma is far less common than granular cell tumor and the granular cytoplasm of granular cell tumor may mimic rhabdomyoma. However, granular cell tumor 20 should not have the fine cytoplasm as adult rhabdomyoma and they should not contain striations. Also, "spider cells" and large cytoplasmic vacuoles should not be a prominent feature in granular cell tumor. Immunohistochemistry, granular cell tumors are positive for S100 proteins and markers that highlight lysosomes such as CD68 and negative for desmin and other striated muscle markers. The cytoplasm of granular cell tumor is PAS positive and diastase resistant. In contrast, rhabdomyomas are positive for desmin and muscle specific actin and less commonly for S100, vimentin, and Leu-7. Adult rhabdomyoma may contains some glycogen that is positive for PAS and diastase sensitive. The cytoplasm, however, is negative for PAS.
The other less common entities for differential diagnosis include hibernoma which are characterized with numerous small cytoplasmic vacuoles, and crystal-storing histiocytosis associated with lymphoplasmacytic neoplasm 21, 22. The crystal storing histiocytes are positive for PAS and CD68 but negative for skeletal muscle markers and S-100 protein. Paraganglioma should also be considered and paragangliomas are positive for synpatophysin and contains S100 positive sustantecular cells.
References:
Kapadia SB, Meis JM, Frisman DM, Ellis GL, Heffner DK, Hyams VJ. Adult rhabdomyoma of the head and neck: a clinicopathologic and immunophenotypic study. Hum Pathol. 1993 Jun;24(6):608-17.
Huang X, Yang X, Wang Z, Li W, Jiang W, Chen X, Hu Q. Adult rhabdomyoma of the tongue in a child. Pathology. 2012 Jan;44(1):51-3.
Catalfamo L, Lombardo G, Siniscalchi EN, Nava C, Familiari E, Francesco Sde P. Rhabdomyomas of the submandibular and sublingual glands. J Craniofac Surg. 2010 May;21(3):927-30.
Papaspyrou G, Werner JA, Roessler M, Devaney KO, Rinaldo A, Ferlito A. Adult rhabdomyoma in the parapharyngeal space: report of 2 cases and review of the literature. Am J Otolaryngol. 2011 May-Jun;32(3):240-6. Epub 2010 Apr 13.
Karaman E, Saritzali G, Ozcora E. Rhabdomyoma of the tonsillar fossa. J Craniofac Surg. 2009 Jul;20(4):1207-9.
Brys AK, Sakai O, DeRosa J, Shapshay SM. Rhabdomyoma of the larynx: case report and clinical and pathologic review. Ear Nose Throat J. 2005 Jul;84(7):437-40.
Bjørndal Sørensen K, Godballe C, Ostergaard B, Krogdahl A. Adult extracardiac rhabdomyoma: light and immunohistochemical studies of two cases in the parapharyngeal space. Head Neck. 2006 Mar;28(3):275-9.
Hansen T, Katenkamp D. Rhabdomyoma of the head and neck: morphology and differential diagnosis. Virchows Arch. 2005 Nov;447(5):849-54.
Vuong PN, Neveux Y, Balaton A, Pham-Thominet L, Houissa-Vuong S, Schoonaert MF, Fombeur JP. Adult-type rhabdomyoma of the palate. Cytologic presentation of two cases with histologic and immunologic study. Acta Cytol. 1990 May-Jun;34(3):413-9.
Zolota V, Tzelepi V, Charoulis N, Apostolakis E, Dougenis D. Mediastinal rhabdomyoma: case report and review of the literature. Virchows Arch. 2006 Jul;449(1):124-8.
Sidhu JS, Nicolas MM, Taylor W. Mediastinal rhabdomyoma: a case report and review of the literature. Int J Surg Pathol. 2002 Oct;10(4):313-8.
Liess BD, Zitsch RP 3rd, Lane R, Bickel JT. Multifocal adult rhabdomyoma: a case report and literature review. Am J Otolaryngol. 2005 May-Jun;26(3):214-7.
Koutsimpelas D, Weber A, Lippert BM, Mann WJ. Multifocal adult rhabdomyoma of the head and neck: a case report and literature review. Auris Nasus Larynx. 2008 Jun;35(2):313-7. Epub 2008 Jan 14.
Etit D, Bayol U, Cumurcu S, Erdogan I, Tan A. Cytology of a giant adult-type rhabdomyoma of the tongue. Diagn Cytopathol. 2011 Sep;39(9):686-8.
Gupta N, Rajwanshi A, Mohindra S, Vasishta RK, Batra C, Gupta AK. Diagnosis of adult rhabdomyoma by fine needle aspiration cytology: a report of 2 cases. Acta Cytol. 2010 Sep-Oct;54(5 Suppl):968-72.
Jin B, Saleh H. Pitfalls in the diagnosis of adult rhabdomyoma by fine needle aspiration: report of a case and a brief literature review. Diagn Cytopathol. 2009 Jul;37(7):483-6.
Truong LD, Rangdaeng S, Cagle P, Ro JY, Hawkins H, Font RL. The diagnostic utility of desmin. A study of 584 cases and review of the literature. Am J Clin Pathol. 1990 Mar;93(3):305-14.
Seidal T, Kindblom LG, Angervall L. Myoglobin, desmin and vimentin in ultrastructurally proven rhabdomyomas and rhabdomyosarcomas. An immunohistochemical study utilizing a series of monoclonal and polyclonal antibodies. Appl Pathol. 1987;5(4):201-19.
Eusebi V, Ceccarelli C, Daniele E, Collina G, Viale G, Mancini AM. Extracardiac rh`abdomyoma: An immunocytochemical study and review of the literature. Appl Pathol. 1988;6(3):197-207.
Rekhi B, Jambhekar NA. Morphologic spectrum, immunohistochemical analysis, and clinical features of a series of granular cell tumors of soft tissues: a study from a tertiary referral cancer center. Ann Diagn Pathol. 2010 Jun;14(3):162-7.
Friedman MT, Molho L, Valderrama E, Kahn LB. Crystal-storing histiocytosis associated with a lymphoplasmacytic neoplasm mimicking adult rhabdomyoma: a case report and review of the literature. Arch Pathol Lab Med. 1996 Dec;120(12):1133-6.
Jones D, Bhatia VK, Krausz T, Pinkus GS. Crystal-storing histiocytosis: a disorder occurring in plasmacytic tumors expressing immunoglobulin kappa light chain. Hum Pathol. 1999 Dec;30(12):1441-8.