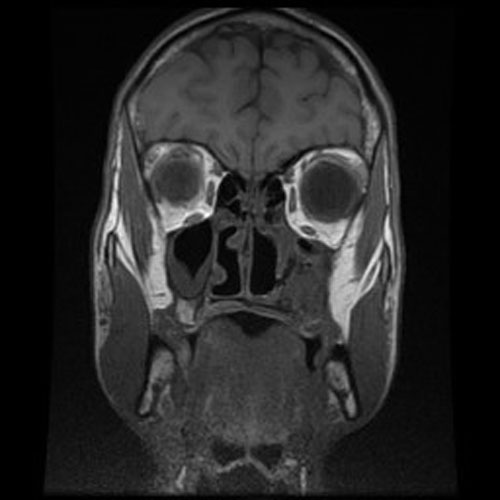
MRI Coronal
A. Hematoxylin & Eosin
B. Hematoxylin & Eosin
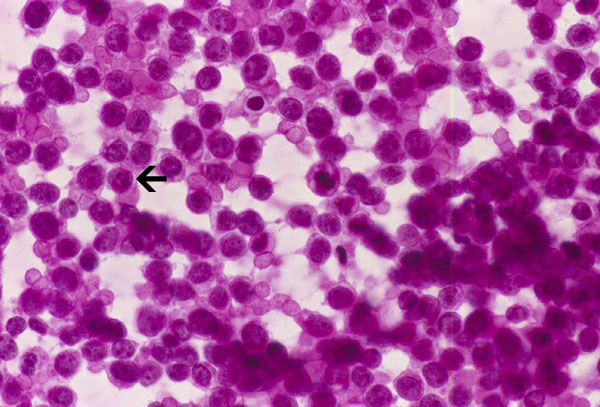
C. Hematoxylin & Eosin
D. PAS stain
E. PAS stain with diastase
F. CD99
G. Synaptophysin
| A 40 year-old Man with Headache, Nausea, and a
Diffusely Infiltrative non-enhancing Lesion. March, 2012, Case 1203-1. Home Page |
Kar-Ming Fung, M.D., Ph.D. Last update: April 20, 2020.
Department of Pathology, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma.
Clinical information: The patient was a 20 year-old man who was referred to this hospital because of a nasal mass. MRI revealed a poorly enhancing mass just posterior to the mucosa of the left maxillary sinus in the region of the pterygoid plates. An endoscopic biopsy was performed and yielded the current specimen. The followings are representative images:
|
MRI Coronal |
A. Hematoxylin & Eosin |
B. Hematoxylin & Eosin |
C. Hematoxylin & Eosin |
|
D. PAS stain |
E. PAS stain with diastase |
F. CD99 |
G. Synaptophysin |
Radiology of the Case: There is an expansile lesion in the left maxillary sinus that invades into the palate and alveolar ridge. This is an aggressive tumor.
Pathology of the Case: Essentially, this is a small blue cell tumor with focal necrosis (Panel A and B). The nuclei are rather monotonous. Please note that the nuclei are slightly larger than most so-called small blue cell tumor such as small cell carcinoma of the lung. The tumor arrange in solid sheets without any pattern formation. There is a gap in between the cells. This is not uncommon in Ewing sarcoma. However, this pattern can also be seen in hematopoietic tumors such as lymphoma and plasmacytoma. In some areas, some of the tumor cells have a small rim of cytoplasm and some of these rims appear to be formed by fused minute bubbles (Arrow in Panel C). Results of speical stains, immunohistochemistry and molecular studies are as follow:
Special Stain:
PAS stain with and without diastase: The tumor cells contains significant amount of cytoplasmic PAS positive material that is sensitive to diastase digestion (Panel D and E).
Immunohistochemistry:
CD99: Positive in tumor cells (Panel F).
Synaptophysin: Positive in some tumor cells (Panel G).
Neuforilament: Positive in scant tumor cells.
CD3, CD20, leukocyte common antigen (LCA): Negative in tumor cells.
S100: Negative in tumor cells.
Cytokeratin AE1/AE3, 7, 20: Negative in tumor cells.
Epithelial membrane antigen (EMA): Negative in tumor cells.
Desmin: Negative in tumor cells.
Molecular Pathology:
Fluorescent in situ hybridization (FISH): A 22 t(11;22) translocation is demosntrated in tumor cells [nuc ish (EWSR1x2)(5'EWSR1sep 3'EWSR1)].
| DIAGNOSIS: Ewing's sarcoma / primitive neuroectodermal tumor (PNET) |
Comment:
With all things being considered, it is likely that this tumor arose from the osseous component of the sinus. However, an extraosseous origin cannot be entirely rule out.
Although Ewing sarcoma is essentially one of the small blue cell tumors which is difficult to diagnose particularly when the clinical information is not known or not typical. However, there are some soft findings that are suggestive of Ewing's sarcoma on histopathologic features alone. One must remember that Ewing sarcoma does not read textbooks and they can arise in many unexpected location such as this case.
First, although it is composed of small blue cells, the nuclei are marginally larger than other small blue cell tumors such as small cell carcinoma or medulloblastoma. Their nuclei are also slightly less crumbled after fixation, less hyperchromatic, and have slightly more open chromatin. A small nucleolus can be seen in many nuclei. The nuclei seems to be more monotonous on cytologic (squash or touch preparation) and crush effects on nuclei (smearing of nuclei) is far less common than other small blue cell tumors. Histologically, it is not uncommon for Ewing's sarcoma to have areas of more densely packed areas with hyperchromatic nuclei and these areas are embedded within a slightly less densely packed area with more open nuclei (Image 1 below). On cytologic preparations, small vacuoles may be present in the cytoplasm. These vacuoles are glycogen granues which could be partially washed out during processing as glycogen has a low aqueous solubility and are typically not entirely washed out during processing (arrow in image 2 below). These vacuoles can be seen in both hematoxylin and eosin stained and Diff-Quick stained cytologic preparations but Diff-Quick works better [Click here to see a case]. Together with the appropriate clinical information, these histologic features are highly suggestive of Ewing's sarcoma.
However, these are only soft evidence. Definitive diagnosis shoud be confirmed by immunohistochemistry and molecular pathology.
|
1. Hematoxylin and eosin stain, permanent section |
Note the densely packed areas with hyperchromatic nuclei embedded in a background of nuclei with less hyperchromatic nuclei. |
|
Note the cytoplasmic vacuoles (arrow). Glycogen does not take up eosin stains. |
Discussion: General Information Pathology Molecular Differential diagnosis Related cases
Ewing sarcoma, also known as
peripheral primitive neuroectodermal tumor, is a malignant,
usually osseous based tumor. Extraosseous presentation is not uncommon.
Histologically, it belongs to the family of small round cell tumor
and genetically characterized by translocation involving the
EWSR1 gene.
EWSR1-FLI1 fusion is most common,
EWSR1-ERG and EWSR1-ETV1
are less common.
With this molecular signature, FISH [Chen
S et al., 2015] or RT-PCR
[Gamberi
G et al., 2011] is often employed to confirm the
diagnosis.
Ewing sarcoma is the third most common
malignant bone tumor after osteosarcoma and chondrosarcoma. Classic presentation
is a malignant primary bone tumor with 80% of cases occurring in the 1st and 2nd
decades of life with a lower incidence in black subjects. Most of the remaining
cases are diagnosed in the 3rd decades but occurrence in older
patients has been documented. Male is more affected.
In a study of 856 cases. Tumor sites
include lower extremity (35%), chest (21%), pelvis (17%),
spine (10%), upper extremity (9%), head and neck (6%), and abdomen (2%)
[Le Deley MC et al., 2014].
Radiographically, intra-osseous Ewing sarcomas appear as poorly-defined,
permeative, osteolytic and destructive lesions. Origin of the tumor in our case
cannot be pinpointed but it probably arise from the bone in the maxillary sinus.
So this case cannot be considered exactly extraskeletal although the bulk of the
tumor is in the sinus space.
One must know that Ewing sarcoma
may occur in any deep soft tissue of the extremities, mostly upper thigh and
buttock, upper arm and shoulder with rare case occurring in the retroperitoneum.
It can also occur in internal organs interning parotid
[Gulsen S & Vicdan H, 2019], kidney
[Bradford K et al., 2020],
intra-cranial locations [VandenHeuvel KA et al., 2015]
and many other extraskeletal locations. Ewing sarcomas are well documented in
the head and neck region [Olson MD, 2018]
including the orbit [Kaliki S, 2018]
and intracranial locations [VandenHeuvel KA et al., 2015].
With all of these cases taken into consideration, extraskeletal Ewing sarcoma
may be more common than expected. Histologically, Ewing sarcoma is a small round
cell tumor that can be mimicked by many other tumors. As extraskeletal Ewing
sarcomas are uncommon in reference to its mimickers, a high index of suspicion
is the first line of defense for correct diagnosis. In brief, Ewing sarcoma is
an important differential diagnosis in extraskeletal, particularly in deep soft
tissue.
Ewing sarcoma occurring in the
head and neck area tends to occur in slightly older patients with a median of 21
years of age. Most of them were associated with the cervical spine and skull
with only 3 out of 17 cases occurred in the sinuses according to one study
[Olson MD, 2018].
Mandibular cases have also been described [Takami
Y, 2020;
Oliveira SV 2019;
Petrovic I et al., 2019].
The 5-year overall survival and recurrence free survival is 87% and 75%
respectively [Olson MD, 2018].
In the orbital cases, 4 out of the 12 cases are 20 years of age or older
[Kaliki S, 2018].
Outcome of these cases are poor with disease-related death occuring in 92% of
the cases within the first 28 months of follow up with only one long term
survival case (alive at 152 months of follow up). In skeletal cases, the 5-year
survival rate with treatment is about 70%.
Ewing sarcoma belongs to the
family of non-hematologic small round cell tumor characterize by small,
undifferentiated, cells with hyperchromatic nuclei. Rosettes similar to Homer
Wright rosettes are occasionally present but tumor cells usually arrange in
solid sheets. Densely packed solid sheets of small round cells with minimal to
no interlacing collagenous collagen or stromal component is the classic
appearance. These tumors are richly vascularized by a delicate network but it is
not obvious because of compression of vessels by tumor cells. Typically, no
inflammatory cells are present. Necrosis is a typically present.
Tumor cells are fairly uniform
and have a small amount of cytoplasm typically in the form of a thin rim.
Intercellular gaps that are often seen in hematopoietic neoplasms may be
present. Cytoplasmic vacuoles corresponding to the glycogen vacuoles can be well
appreciated in cytologic preparations. However, it is hard to differentiate them
from fixation artifacts in permanent sections. Ewing sarcoma typically contains
a good amount of glycogen that are well demonstrated by PAS stain with and
without diastase pre-digestion. The nuclear chromatin is finely granular.
Although it is a small round cell tumor, its nuclei tend to be marginally larger
and less crumbled than many of the other small round cell tumors such as small
cell carcinoma. It is common to have geographic patches of cells with open
chromatin alternating with areas with closed chromatin leading to a biphasic
dark cells and light cells pattern. Small but identifiable small to moderately
sized nucleoli. Large and prominent nucleoli can be seen in large cell Ewing
sarcoma. Otherwise, large and prominent nucleoli are not typical for Ewing
sarcoma.
Within this general layout, there is Ewing sarcomas do demonstrate a spectrum of pathologic features. In a study of 415 cases,
putative transcriptional target of
EWSR1-FLI1, is highly specific in recognizing Ewing sarcoma from its
mimickers. NKX2.2
is positive in Ewing sarcoma
[Hung YP et al., 2016;
McCuiston A et al., 2018]. In one study, it
is expressed in 80% of Ewing sarcoma but only 16% of its mimickers
[Shibuya R et al., 2014]. Nuclear immunoreactivity
of FLI1 has been demonstrated in 70% to 90% of Ewing sarcomas including cases
with the less common EWSR-1ERG fusion
[.
The following markers are not useful in establishing the diagnosis but they are helpful in differentiating Ewing sarcoma from its mimickers. Synaptophysin is weakly positive in Ewing sarcoma and is also positive for other neural specific markers including CD57, S100 protein, and PGP9.5. About 25% of Ewing sarcomas express keratin, usually low molecular weight keratin, except for adamantinoma-like variant which diffusely express keratin including high molecular weight keratin. The adamantinoma-like variant can also express p40. Ewing sarcoma can also express desmin but not MyoD and myogenin which distinguishes them from alveolar rhabdomyosarcoma.
The
molecular pathology of Ewing sarcoma and related tumors is well reviewed by
Antonescu C, (2014). The molecular signature of Ewing sarcoma is a nonrandom
translocation leading to fusion of the EWSR1 gene and one of the several members
of the ETS family of transcription factors. Reciprocal t(11;22)(q24;q12)
translocation resulting a chimeric EWSR1-FLI1 fusion protein is present in about 85% of cases.
EWSR1-ERG
and EWSR1-ETV1 are less common
[Source]. EWSR1 on 22q12, in fact, can partner with several other different
gene by reciprocal translocation and these fusion genes are noted in a variety
of malignancy including acute leukemia (EWSR1-ZNF384),
myxoid liposarcoma (EWSR1-DDIT3),
extraskeletal myxoid chondrosarcoma (EWSR1-NR4A3),
desmoplastic small round cell tumor (EWSR1-sEGR),
and others [Source].
FISH or
RT-PCR is typically employed to confirm diagnoses of Ewing sarcoma. A small
amount of Ewing sarcoma show FUS gene
arrangement instead of EWSR1
rearrangement [de Alava E, 2017;
Chen S et al., 2016;
Antonescu C, 2014;
Antonescu CR & Dal Cin P, 2014].
FISH study on
EWSR1 rearrangement is not fool proof for the diagnosis of Ewing
sarcoma. The molecular results should be interpreted with the histopathologic
and immunohistochemical findings as EWSR1
and FUS gene arrangements occur in
many other tumors.
First and foremost, all of these
mimickers lack the characteristic gene fusions of Ewing sarcoma.
Skeletal
and extra-skeletal Ewing sarcomas have a slightly different list of differential
diagnosis than it intraosseous counterpart. The common mimickers of skeletal Ewing sarcoma include metastatic
neuroblastoma, hematopoietic malignancies, osteosarcoma with small cell
component, metastatic small cell carcinoma and adamantinoma.
Extraskeletal Ewing sarcoma are most common in deep soft tissues. Mimickers include hematopoietic malignancies particularly lymphoblastic lymphoma. While lymphoblastic lymphoma is positive for CD99, they are also positive for TdT and other hematopoietic markers. Desmoplastic small round cell tumor is cytologically similar to Ewing sarcoma but they are typically associated with fibrosis. Some of these tumors can be positive for CD99 and NKX2.2 but they are also positive for WT1,multiple epithelial marker, and typically with positive dot like immunoreactivity for desmin. Most importantly, desmoplastic small round cell tumors are associated with EWSRI-WT1 fusion. Alveolar rhabdomyosarcoma does not harbor any specific genetic aberration. A small percentage of them are positive for CD99 but they are positive for desmin, myogenin, and MyoD. Primary and metastatic neuroblastomas are strongly positive for synaptophysin. Metastatic small cell carcinoma are strongly positive for synaptophysin and cytokeratins. Monophasic synovial sarcoma can be a diagnostic challenge. Although cellular, synovial sarcoma is a spindle cell tumor but not a small round cell tumor in most of the cases. SS18-SSX1 [Ladanyi M et al., 2002] or SS18-SSX2 [Canter RJ et al., 2008] translocations are typically seen in biphasic and monophasic synovial sarcomas respectively.